

Early Patterns of Macular Degeneration in ABCA4-Associated Retinopathy
- PMID: 29310964
- PMCID: PMC5917070
- DOI: 10.1016/j.ophtha.2017.11.020
Early Patterns of Macular Degeneration in ABCA4-Associated Retinopathy
Abstract
Purpose: To describe the earliest features of ABCA4-associated retinopathy.
Design: Case series.
Participants: Children with a clinical and molecular diagnosis of ABCA4-associated retinopathy without evidence of macular atrophy.
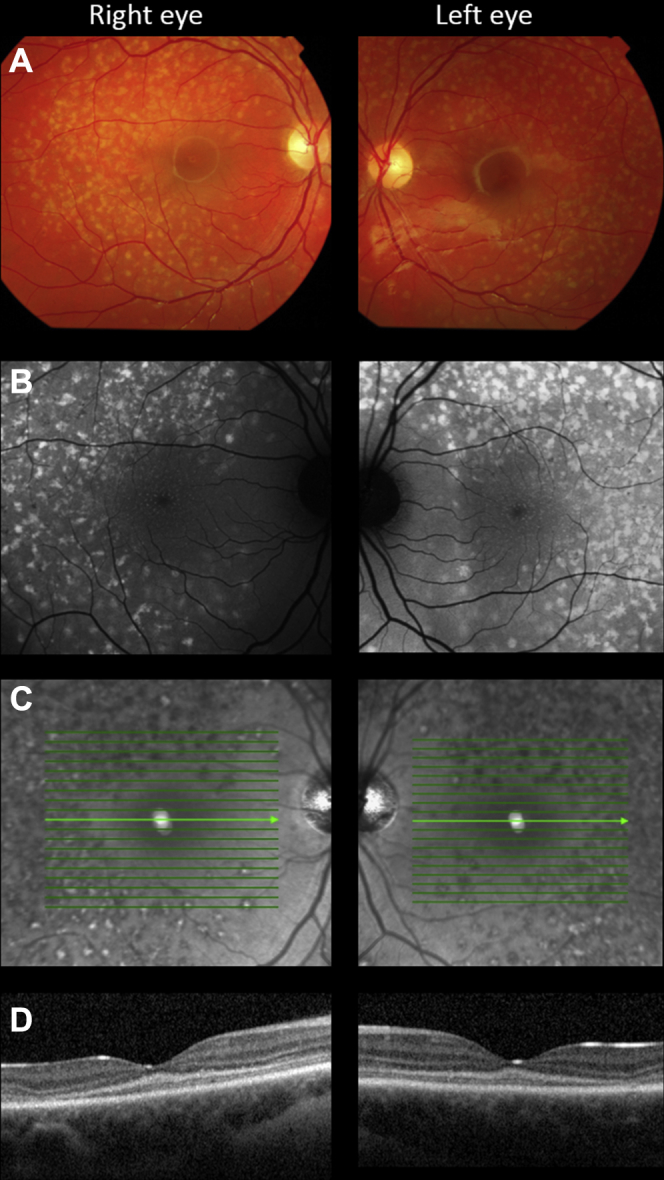
Methods: The retinal phenotype was characterized by color fundus photography, OCT, fundus autofluorescence (FAF) imaging, electroretinography, and in 2 patients, adaptive optics scanning laser ophthalmoscopy (AOSLO). Sequencing of the ABCA4 gene was performed in all patients.
Main outcome measures: Visual acuity, OCT, FAF, electroretinography, and AOSLO results.
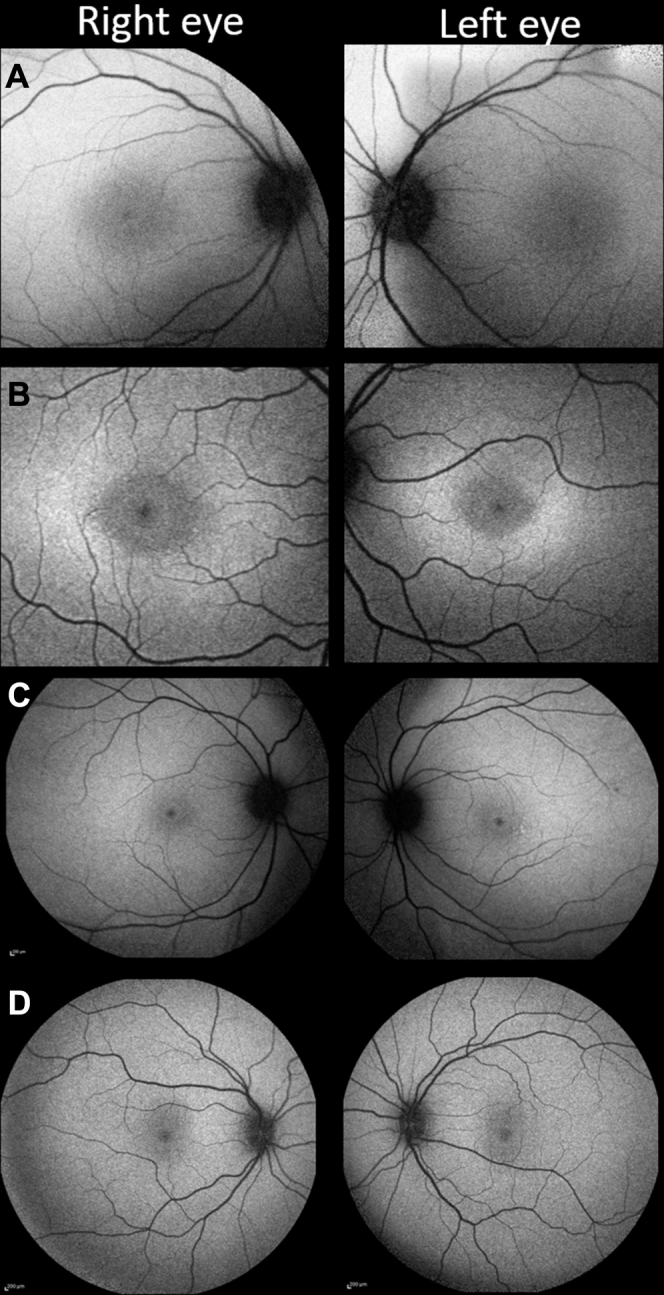
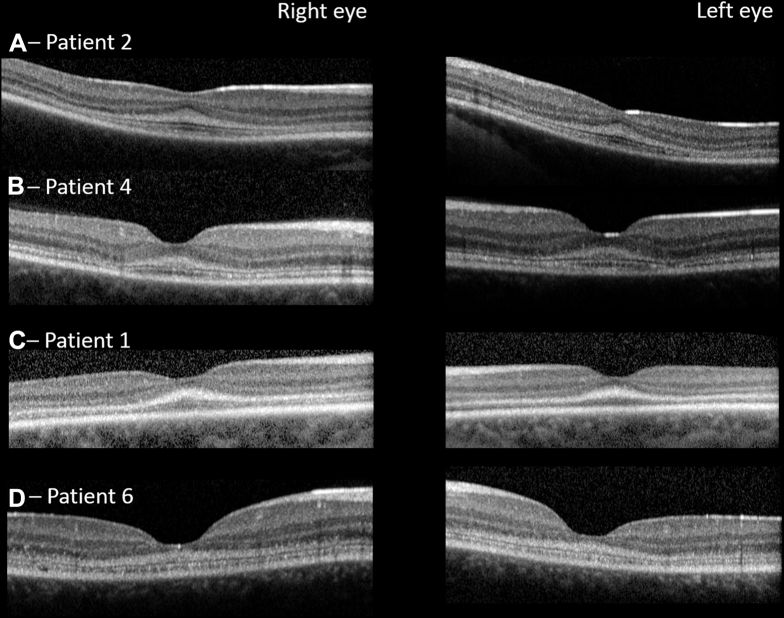
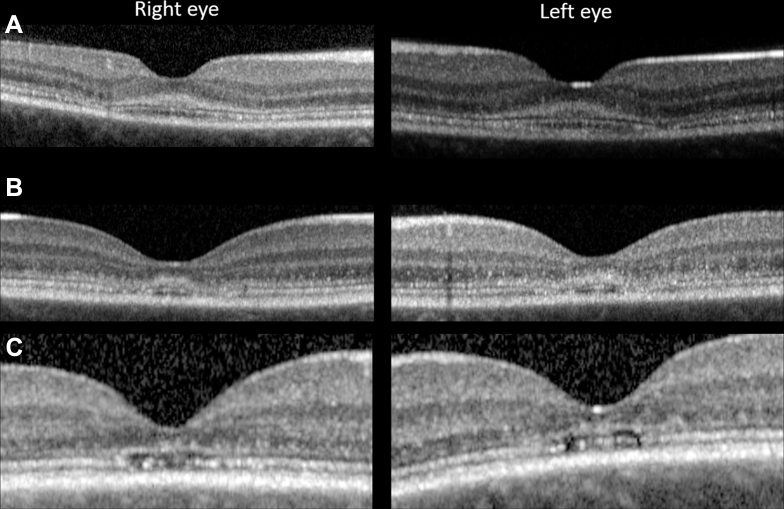
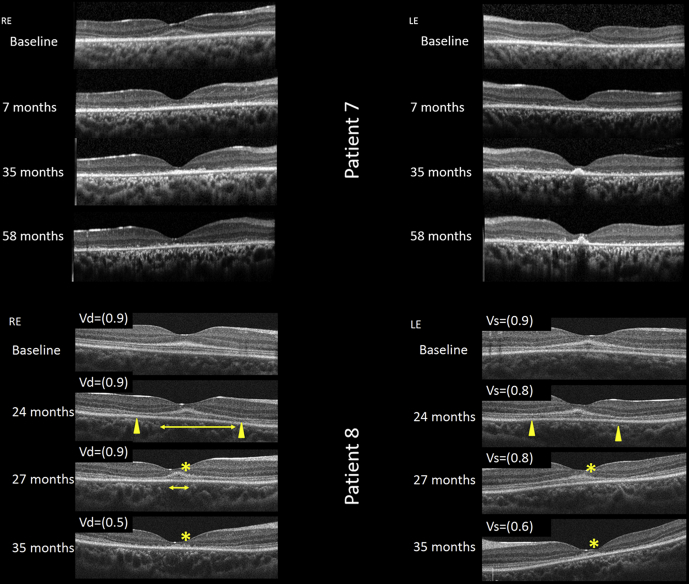
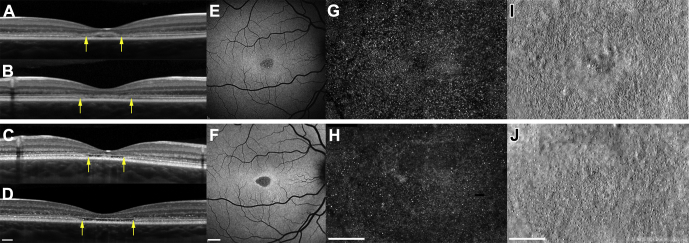
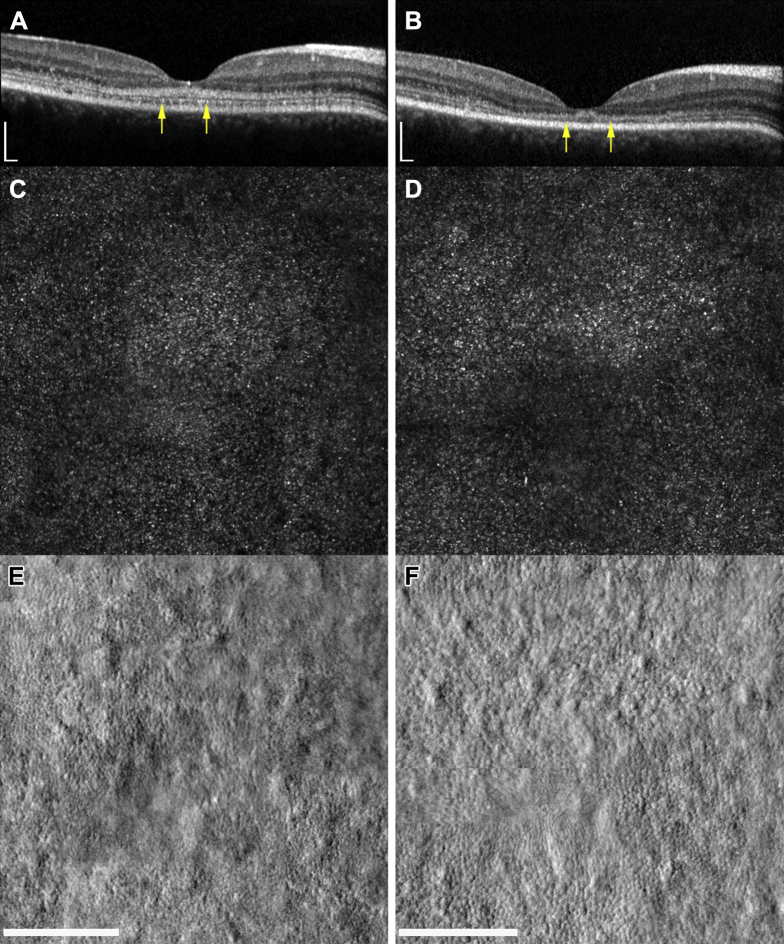
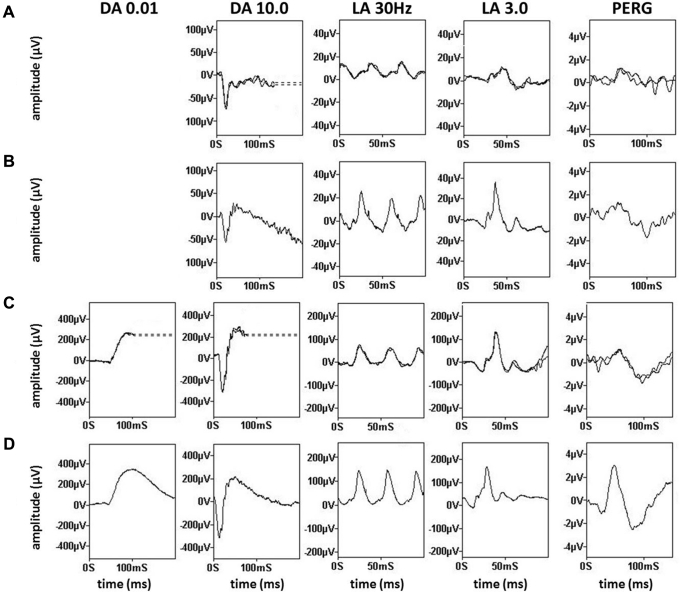
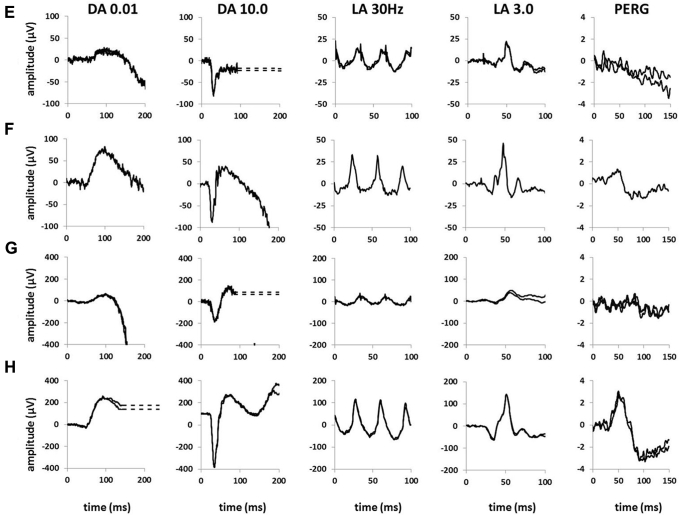
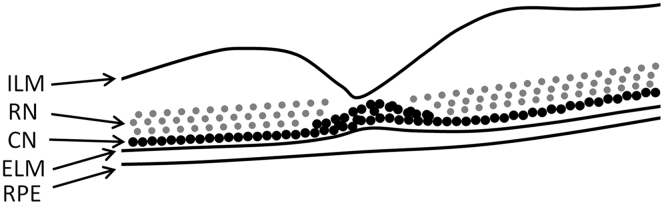
Results: Eight children with ABCA4-associated retinopathy without macular atrophy were identified. Biallelic variants in ABCA4 were identified in all patients. Four children were asymptomatic, and 4 reported loss of VA. Patients were young (median age, 8.5 years; interquartile range, 6.8 years) with good visual acuity (median, 0.155 logarithm of the minimum angle of resolution [logMAR]; interquartile range, 0.29 logMAR). At presentation, the macula appeared normal (n = 3), had a subtly altered foveal reflex (n = 4), or demonstrated manifest fine yellow dots (n = 1). Fundus autofluorescence identified hyperautofluorescent dots in the central macula in 3 patients, 2 of whom showed a normal fundus appearance. Only 1 child had widespread hyperautofluorescent retinal flecks at presentation. OCT imaging identified hyperreflectivity at the base of the outer nuclear layer in all 8 patients. Where loss of outer nuclear volume was evident, this appeared to occur preferentially at a perifoveal locus. Longitudinal split-detector AOSLO imaging in 2 individuals confirmed that the greatest change in cone spacing occurred in the perifoveal, and not foveolar, photoreceptors. Electroretinography showed a reduced B-wave-to-A-wave ratio in 3 of 5 patients tested; in 2 children, recordings clearly showed electronegative results.
Conclusions: In childhood-onset ABCA4-associated retinopathy, the earliest stages of macular atrophy involve the parafovea and spare the foveola. In some cases, these changes are predated by tiny, foveal, yellow, hyperautofluorescent dots. Hyperreflectivity at the base of the outer nuclear layer, previously described as thickening of the external limiting membrane, is likely to represent a structural change at the level of the foveal cone nuclei. Electroretinography suggests that the initial site of retinal dysfunction may occur after phototransduction.
Copyright © 2018 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lois N., Holder G.E., Bunce C. Phenotypic subtypes of Stargardt macular dystrophy-fundus flavimaculatus. Arch Ophthalmol. 2001;119:359–369. - PubMed
-
- van Huet R.A., Bax N.M., Westeneng-Van Haaften S.C. Foveal sparing in Stargardt disease. Invest Ophthalmol Vis Sci. 2014;55:7467–7478. - PubMed
-
- Crone J., Pfaffle R., Stobbe H. Familial combined pituitary hormone deficiency caused by PROP-1 gene mutation. Growth patterns and MRI studies in untreated subjects. Horm Res. 2002;57:120–126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
