

Hippocampal dysfunction in the pathophysiology of schizophrenia: a selective review and hypothesis for early detection and intervention
- PMID: 29311665
- PMCID: PMC6037569
- DOI: 10.1038/mp.2017.249
Hippocampal dysfunction in the pathophysiology of schizophrenia: a selective review and hypothesis for early detection and intervention
Abstract
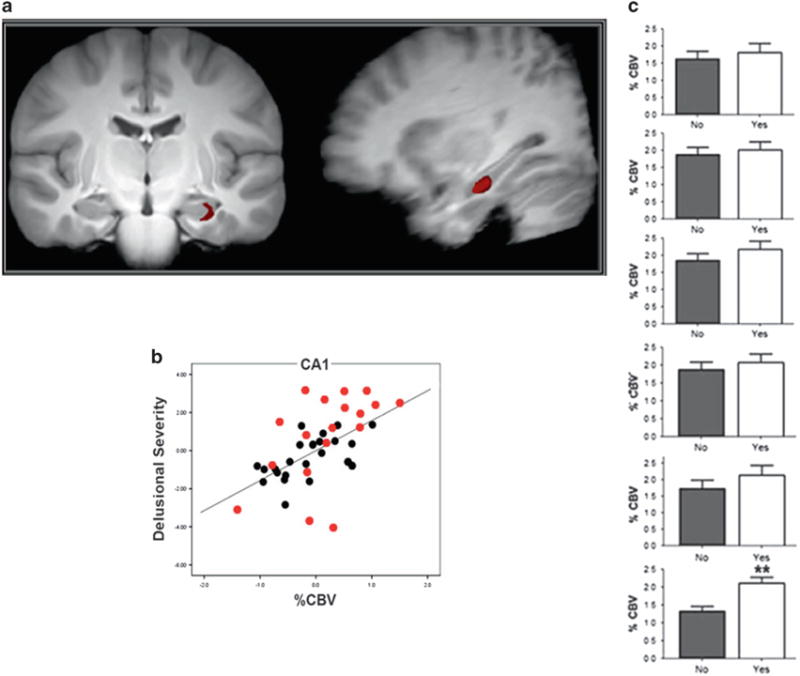
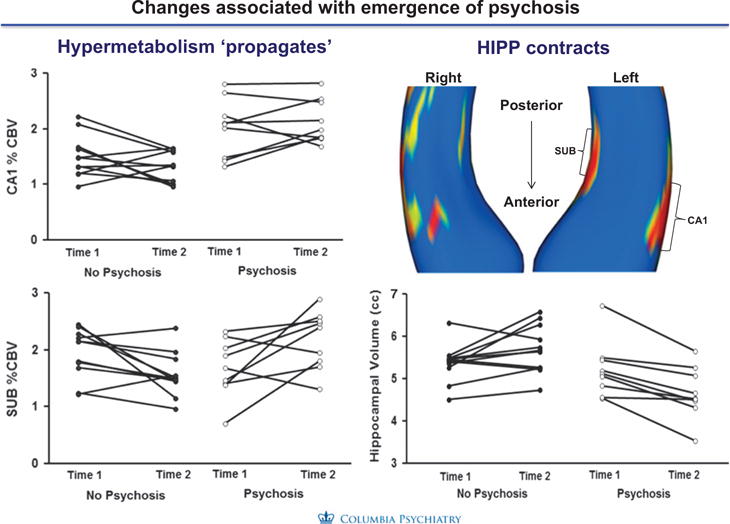
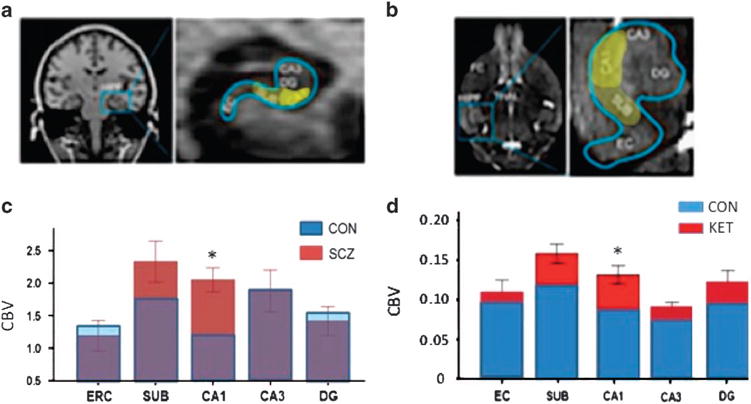
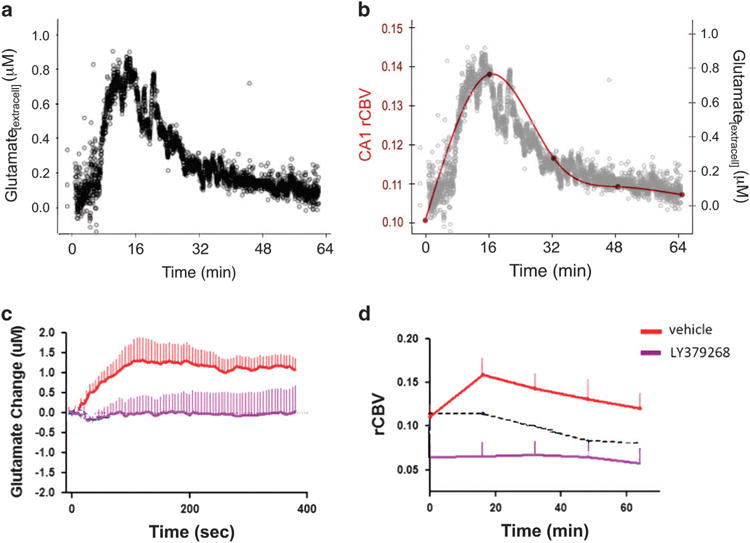
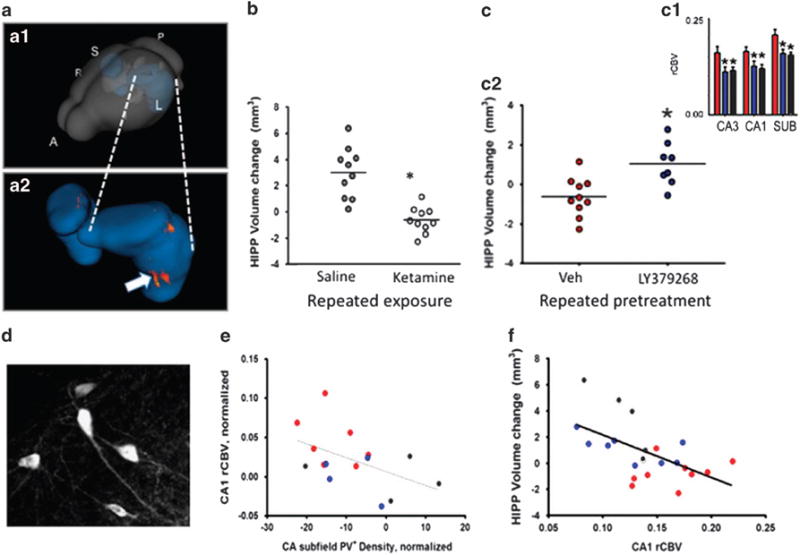
Scientists have long sought to characterize the pathophysiologic basis of schizophrenia and develop biomarkers that could identify the illness. Extensive postmortem and in vivo neuroimaging research has described the early involvement of the hippocampus in the pathophysiology of schizophrenia. In this context, we have developed a hypothesis that describes the evolution of schizophrenia-from the premorbid through the prodromal stages to syndromal psychosis-and posits dysregulation of glutamate neurotransmission beginning in the CA1 region of the hippocampus as inducing attenuated psychotic symptoms and initiating the transition to syndromal psychosis. As the illness progresses, this pathological process expands to other regions of the hippocampal circuit and projection fields in other anatomic areas including the frontal cortex, and induces an atrophic process in which hippocampal neuropil is reduced and interneurons are lost. This paper will describe the studies of our group and other investigators supporting this pathophysiological hypothesis, as well as its implications for early detection and therapeutic intervention.
Conflict of interest statement
Dr. Lieberman (JAL) has received support administered through his institution in the form of funding or medication supplies for investigator initiated research from Denovo, Taisho, Pfizer, Sunovion and Genentech, and for company sponsored phase II, III and IV studies from Alkermes and Allergan, and is a consultant to or member of the advisory board of Intracellular Therapies, Lilly, Pierre Fabre and Psychogenics. He neither accepts nor receives any personal financial remuneration for consulting, speaking or research activities from any pharmaceutical, biotechnology or medical device companies. He has received honoraria for serving on an advisory board for Clintara, a clinical research organization, and holds a patent from Repligen that yields no royalties. Dr. Lieberman has received support administered through his institution in the form of funding or medication supplies for investigator initiated research from Denovo, Taisho, Pfizer, Sunovion and Genentech, and for company sponsored phase II, III and IV studies from Alkermes and Allergan, and is a consultant to or member of the advisory board of Intracellular Therapies, Lilly, Pierre Fabre and Psychogenics. He neither accepts nor receives any personal financial remuneration for consulting, speaking or research activities from any pharmaceutical, biotechnology or medical device companies. He has received honoraria for serving on an advisory board for Clintara, a clinical research organization, and holds a patent from Repligen that yields no royalties. Dr. Girgis (RRG) has received research support from Otsuka, Genentech, Allergan and Bioadvantex. Dr. Small (SAS) is a member of the advisory board for Janssen Pharmaceutical, Denali Therapeutics and Meira GTx. Drs. Brucato (GB), Javitt (DJ), Kegeles (LK), Kantrowitz (JK), Corcoran (CMC), Moore (HM), Provenzano (FP), Schobel (SAS) and Wall (MMW) declare no conflict of interest.
Figures
References
-
- Lewis DA, Hashimoto T, Volk DW. Cortical inhibitory neurons and schizophrenia. Nat Rev Neurosci. 2005;6:312–324. - PubMed
-
- Benes FM. Evidence for altered trisynaptic circuitry in schizophrenic hippocampus. Biol Psychiatry. 1999;46:589–599. - PubMed
-
- Bogerts B, Ashtari M, Degreef G, Alvir JM, Bilder RM, Lieberman JA. Reduced temporal limbic structure volumes on magnetic resonance images in first episode schizophrenia. Psychiatry Res. 1990;35:1–13. - PubMed
-
- Kendler KS. What psychiatric genetics has taught us about the nature of psychiatric illness and what is left to learn. Mol Psychiatry. 2013;18:1058–1066. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
