

Endovascular Thrombectomy for Ischemic Stroke Increases Disability-Free Survival, Quality of Life, and Life Expectancy and Reduces Cost
- PMID: 29312109
- PMCID: PMC5735082
- DOI: 10.3389/fneur.2017.00657
Endovascular Thrombectomy for Ischemic Stroke Increases Disability-Free Survival, Quality of Life, and Life Expectancy and Reduces Cost
Abstract
Background: Endovascular thrombectomy improves functional outcome in large vessel occlusion ischemic stroke. We examined disability, quality of life, survival and acute care costs in the EXTEND-IA trial, which used CT-perfusion imaging selection.
Methods: Large vessel ischemic stroke patients with favorable CT-perfusion were randomized to endovascular thrombectomy after alteplase versus alteplase-only. Clinical outcome was prospectively measured using 90-day modified Rankin scale (mRS). Individual patient expected survival and net difference in Disability/Quality-adjusted life years (DALY/QALY) up to 15 years from stroke were modeled using age, sex, 90-day mRS, and utility scores. Level of care within the first 90 days was prospectively measured and used to estimate procedure and inpatient care costs (US$ reference year 2014).
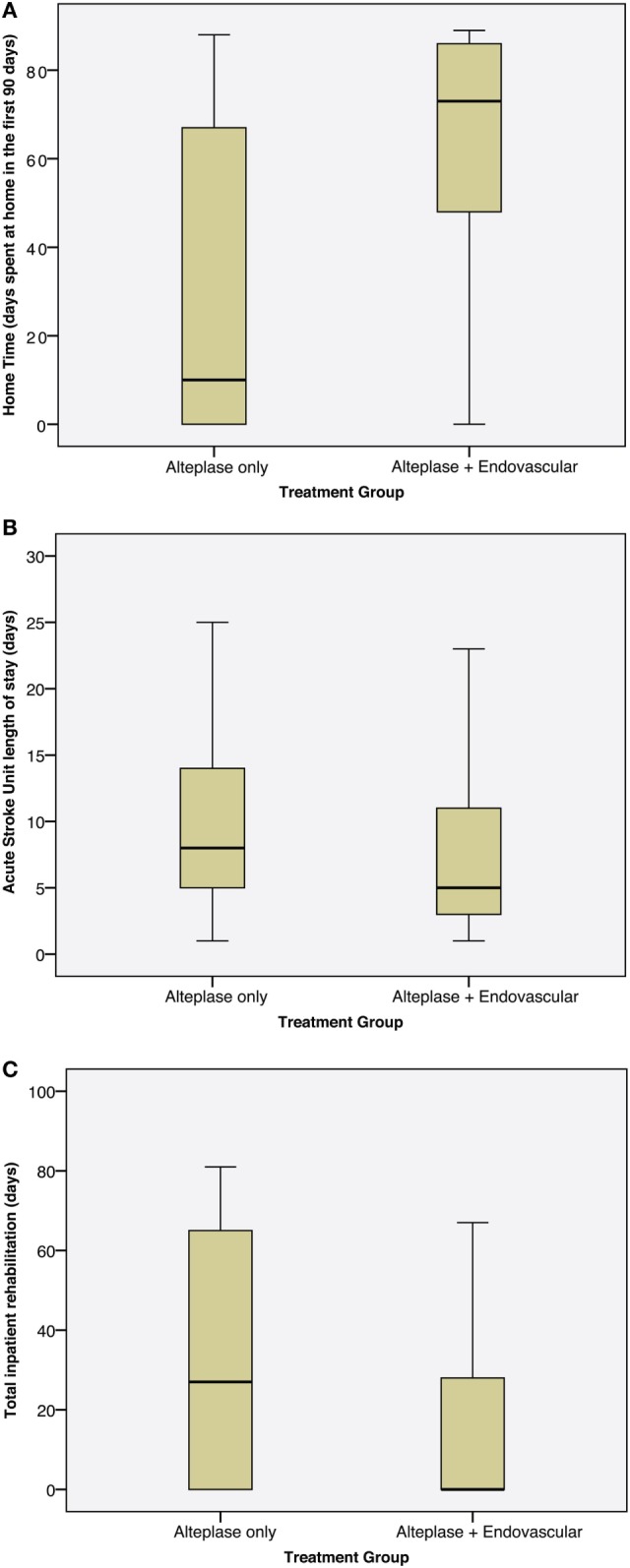
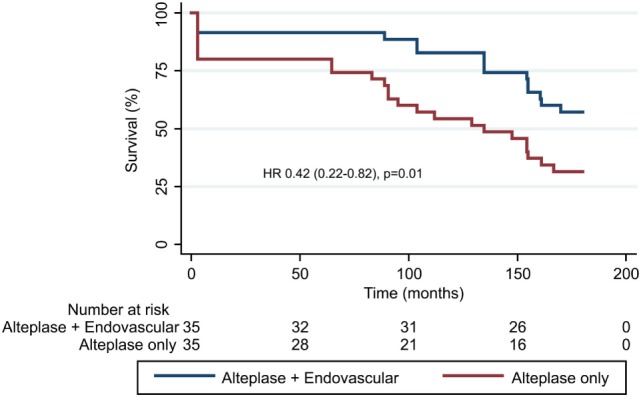
Results: There were 70 patients, 35 in each arm, mean age 69, median NIHSS 15 (IQR 12-19). The median (IQR) disability-weighted utility score at 90 days was 0.65 (0.00-0.91) in the alteplase-only versus 0.91 (0.65-1.00) in the endovascular group (p = 0.005). Modeled life expectancy was greater in the endovascular versus alteplase-only group (median 15.6 versus 11.2 years, p = 0.02). The endovascular thrombectomy group had fewer simulated DALYs lost over 15 years [median (IQR) 5.5 (3.2-8.7) versus 8.9 (4.7-13.8), p = 0.02] and more QALY gained [median (IQR) 9.3 (4.2-13.1) versus 4.9 (0.3-8.5), p = 0.03]. Endovascular patients spent less time in hospital [median (IQR) 5 (3-11) days versus 8 (5-14) days, p = 0.04] and rehabilitation [median (IQR) 0 (0-28) versus 27 (0-65) days, p = 0.03]. The estimated inpatient costs in the first 90 days were less in the thrombectomy group (average US$15,689 versus US$30,569, p = 0.008) offsetting the costs of interhospital transport and the thrombectomy procedure (average US$10,515). The average saving per patient treated with thrombectomy was US$4,365.
Conclusion: Thrombectomy patients with large vessel occlusion and salvageable tissue on CT-perfusion had reduced length of stay and overall costs to 90 days. There was evidence of clinically relevant improvement in long-term survival and quality of life.
Clinical trial registration: http://www.ClinicalTrials.gov NCT01492725 (registered 20/11/2011).
Keywords: CT perfusion; Solitaire stent retriever device; endovascular therapy; intraarterial therapy; ischemic stroke; mechanical thrombectomy; randomized trial; thrombolysis.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical