

Retrospective review of the diagnosis and treatment of pulmonary sequestration in 28 patients: surgery or endovascular techniques?
- PMID: 29312721
- PMCID: PMC5756952
- DOI: 10.21037/jtd.2017.10.145
Retrospective review of the diagnosis and treatment of pulmonary sequestration in 28 patients: surgery or endovascular techniques?
Abstract
Background: Pulmonary sequestration (PS) is a rare congenital pulmonary malformation. In this study, we aimed to retrospect and evaluate the diagnosis, treatment, and outcomes of PS in 28 patients at our institute.
Methods: The files of 28 patients with PS who were treated with surgery (21 cases) or endovascular intervention (7 cases) between May 2005 and June 2016 from a single institute were retrospectively reviewed. The following data of all patients were analyzed: age, sex, clinical symptoms, diagnostic methods, operative techniques, and treatment outcomes.
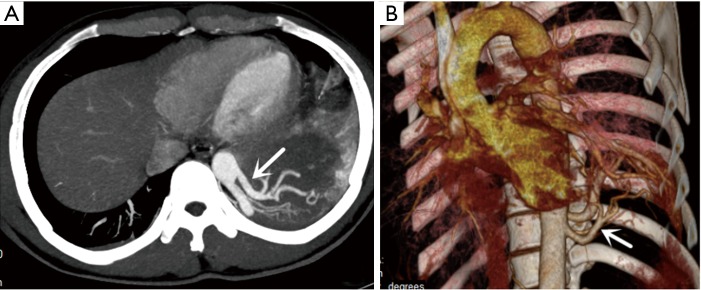
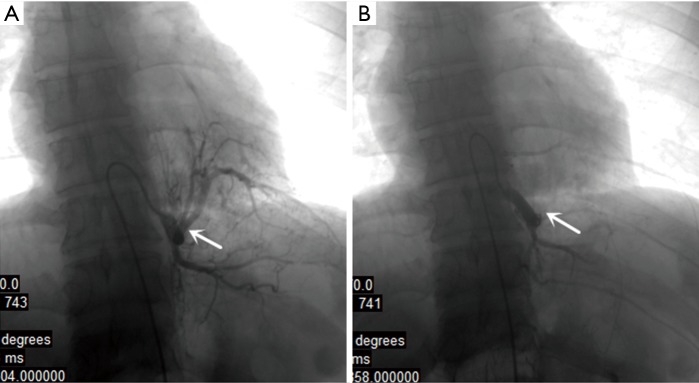
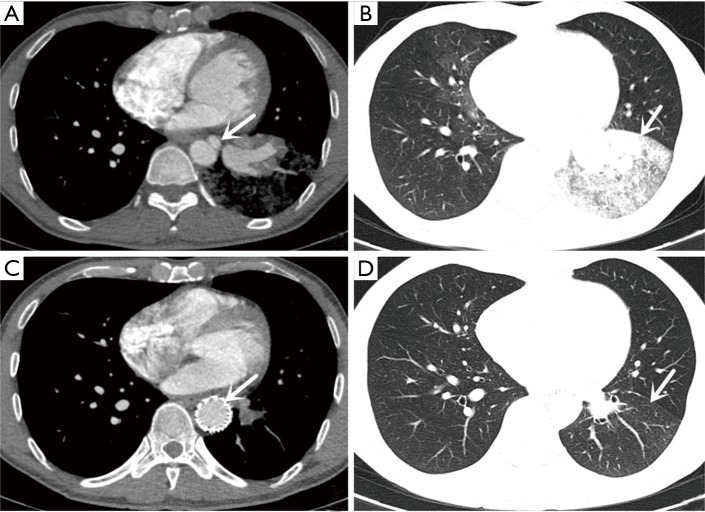
Results: Twenty-eight patients, 15 male and 13 female, with a median age of 42.5 underwent operative intervention for PS. Twenty-one patients showed preoperative symptoms including cough, expectoration, hemoptysis, chest and/or back pain, and fever. General chest computed tomography (CT) scanning; percutaneous needle biopsy, bronchoscopy, enhanced CT scanning, and CT angiography (CTA) were used as diagnostic methods. Twenty-one patients were diagnosed preoperatively by enhanced CT scanning and CTA; seven patients were confirmed by surgery. Twenty-one patients underwent surgery (15 cases via thoracotomy and 6 cases via video-assisted thoracic surgery), seven patients underwent interventional therapy (three cases via endovascular embolization and four cases via thoracic aortic endovascular stent-graft exclusion). Three patients had a complication in surgery group (intraoperative hemorrhage in two patients and postoperative hydropneumothorax in one patient) and two patients had post-embolization syndrome in interventional group (fever and pain at embolism site). During the follow-up period ranging from 6 to 84 months, no recurrences or further complications were observed in two groups.
Conclusions: Enhanced CT or CTA may be a potential approach for the diagnosis of PS. Surgical resection for PS is the major treatment approach. Endovascular embolization of PS could be considered when pulmonary lesion is small-sized. Endovascular exclusion could be used to treat combined arterial aneurysm and dissection of PS.
Keywords: Pulmonary sequestration (PS); intervention therapy; surgery.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources