

Disease-free survival improved by use of adjuvant EGFR tyrosine kinase inhibitors in resectable non-small cell lung cancer: an updated meta-analysis
- PMID: 29312741
- PMCID: PMC5757008
- DOI: 10.21037/jtd.2017.12.58
Disease-free survival improved by use of adjuvant EGFR tyrosine kinase inhibitors in resectable non-small cell lung cancer: an updated meta-analysis
Abstract
Background: A previous meta-analysis of our research team suggested survival advantage from epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) after surgery in patients with EGFR-mutant non-small cell lung cancer (NSCLC). This study aims to follow up on the findings of the previous one and presents our latest updates through the past few years.
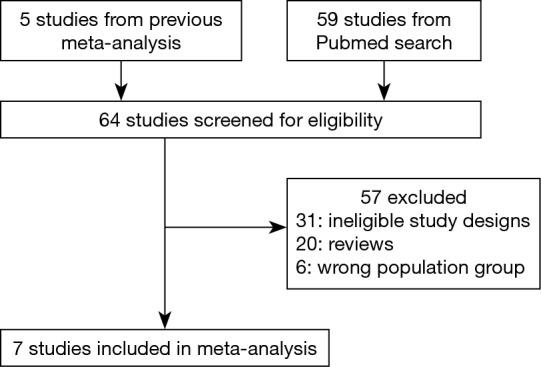
Methods: The study advanced the previous meta-analysis and included a comprehensive range of relevant studies in PubMed. Disease-free survival (DFS) with hazard ratios (HRs) was calculated using random and/or fixed-effects models. Subgroup analysis and meta-regression analysis were also performed.
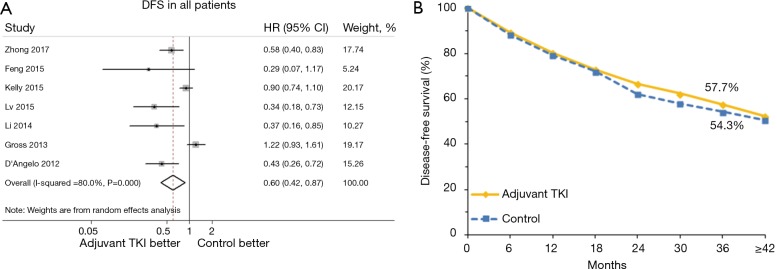
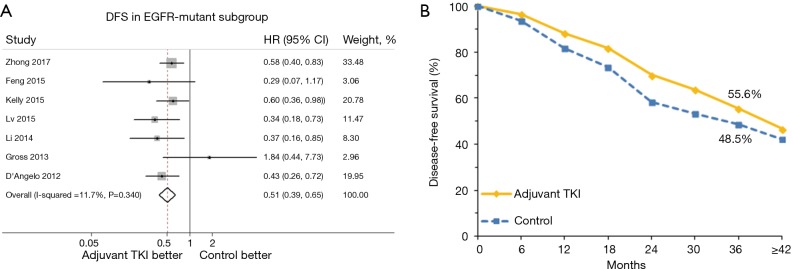
Results: A total of 2,223 patients in seven studies were eligible for the analysis. Adjuvant EGFR-TKIs administration was significantly associated with superior DFS [HR, 0.60; 95% confidence interval (CI), 0.42-0.87], corresponding to an absolute benefit of 3.4% at 3 years, yet with significant heterogeneity (I2=80.0%, P <0.001). EGFR mutation rate of included patients was found to be a source of heterogeneity by meta-regression analysis (P=0.005). In the EGFR-mutant sub-population, HR for DFS was 0.51 (95% CI, 0.39-0.65), corresponding to an absolute benefit of 7.1% at 3 years. The rate of overall grade 3 or greater adverse events (AEs) was 38.9% (95% CI, 35.9-41.9%).
Conclusions: The updated meta-analysis provided strengthened evidence of significant DFS advantage of adjuvant EGFR-TKI treatment for patients with EGFR-mutant NSCLC after complete resection.
Keywords: Epidermal growth factor receptor (EGFR); adjuvant treatment; lung cancer; survival; tyrosine kinase inhibitor (TKI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Rami-Porta R, Bolejack V, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2015;10:990-1003. - PubMed
-
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2012;13:239-46. 10.1016/S1470-2045(11)70393-X - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous