

Acute rejection
- PMID: 29312755
- PMCID: PMC5757020
- DOI: 10.21037/jtd.2017.11.83
Acute rejection
Erratum in
-
Erratum to acute rejection.J Thorac Dis. 2018 Feb;10(2):E165. doi: 10.21037/jtd.2018.01.136. J Thorac Dis. 2018. PMID: 29608201 Free PMC article.
Abstract
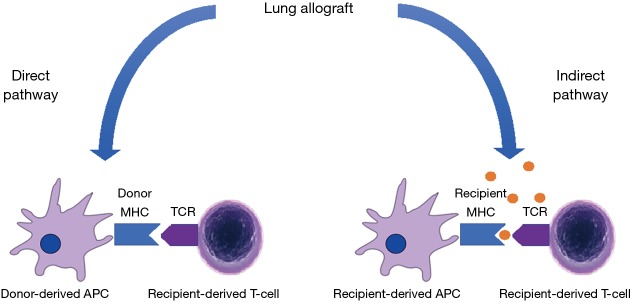
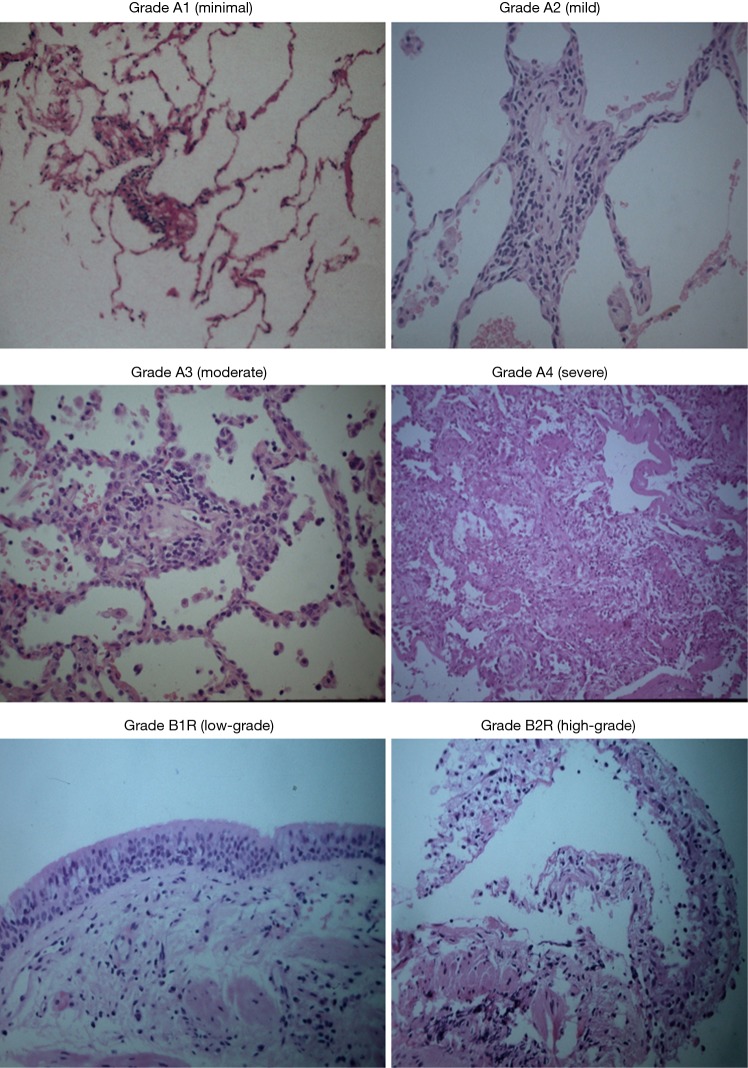
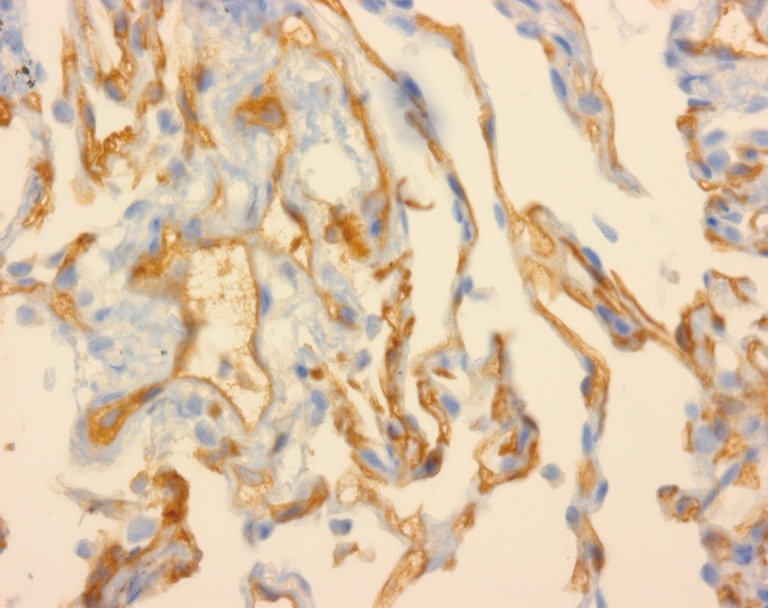
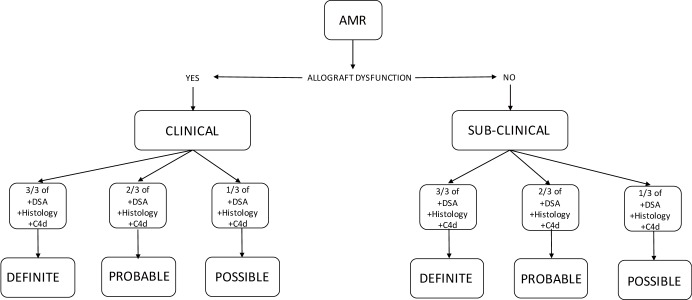
Despite induction immunosuppression and the use of aggressive maintenance immunosuppressive regimens, acute allograft rejection following lung transplantation is still a problem with important diagnostic and therapeutic challenges. As well as causing early graft loss and mortality, acute rejection also initiates the chronic alloimmune responses and airway-centred inflammation that predispose to bronchiolitis obliterans syndrome (BOS), also known as chronic lung allograft dysfunction (CLAD), which is a major source of morbidity and mortality after lung transplantation. Cellular responses to human leukocyte antigens (HLAs) on the allograft have traditionally been considered the main mechanism of acute rejection, but the influence of humoral immunity is increasingly recognised. As with other several other solid organ transplants, antibody-mediated rejection (AMR) is now a well-accepted and distinct clinical entity in lung transplantation. While acute cellular rejection (ACR) has defined histopathological criteria, transbronchial biopsy is less useful in AMR and its diagnosis is complicated by challenges in the measurement of antibodies directed against donor HLA, and a determination of their significance. Increasing awareness of the importance of non-HLA antigens further clouds this issue. Here, we review the pathophysiology, diagnosis, clinical presentation and treatment of ACR and AMR in lung transplantation, and discuss future potential biomarkers of both processes that may forward our understanding of these conditions.
Keywords: Lung transplant; acute antibody rejection; cellular rejection; humoral rejection.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Yusen RD, Edwards LB, Dipchand AI, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Lung and Heart-Lung Transplant Report-2016; Focus Theme: Primary Diagnostic Indications for Transplant. J Heart Lung Transplant 2016;35:1170-84. 10.1016/j.healun.2016.09.001 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials