

Considerations in computer-aided design for inlay cranioplasty: technical note
- PMID: 29313149
- PMCID: PMC5820390
- DOI: 10.1007/s10006-017-0668-4
Considerations in computer-aided design for inlay cranioplasty: technical note
Abstract
Context: Cranioplasty is a frequently performed procedure that uses a variety of reconstruction materials and techniques. In this technical note, we present refinements of computer-aided design-computer-aided manufacturing inlay cranioplasty.
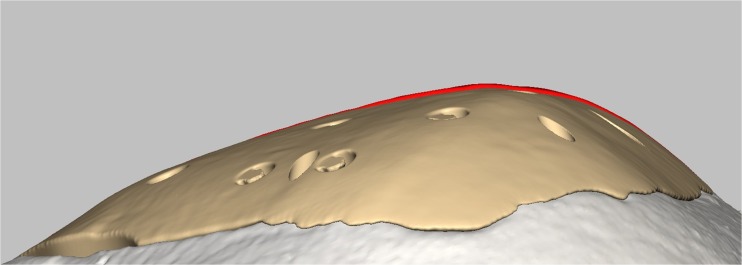
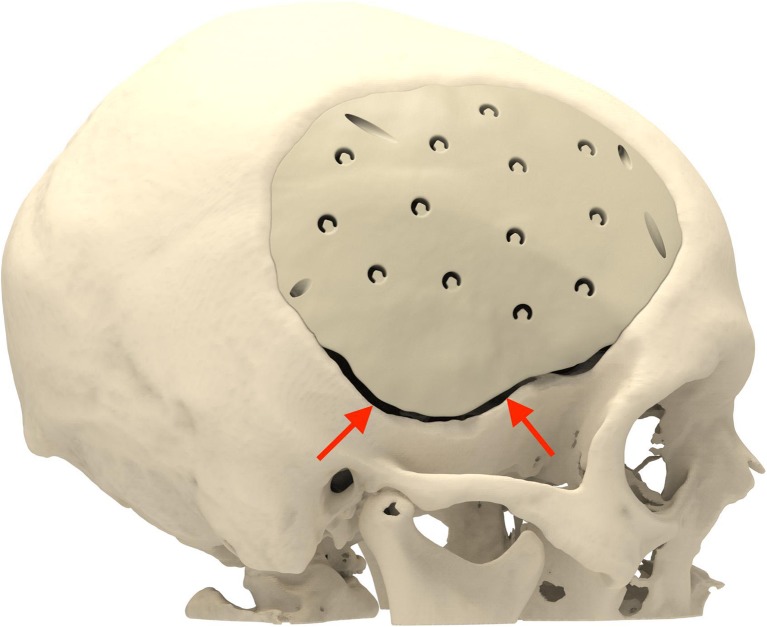
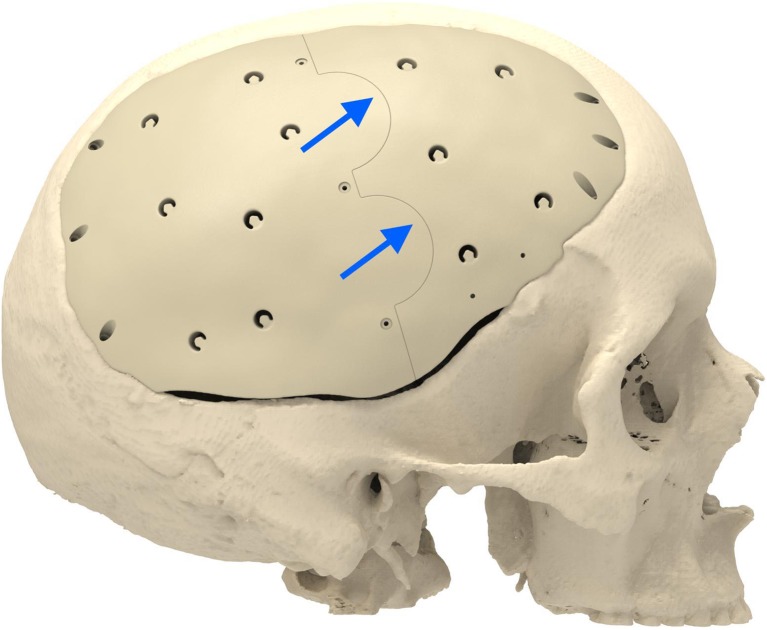
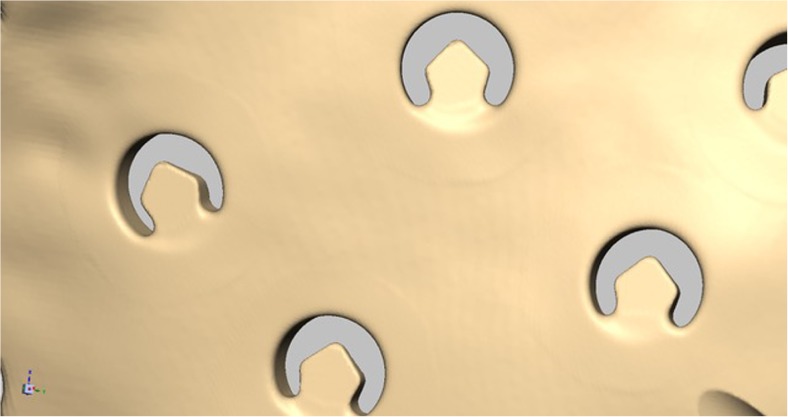
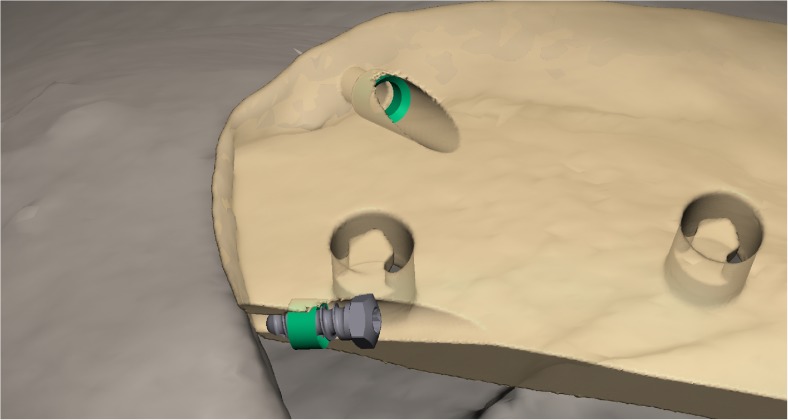
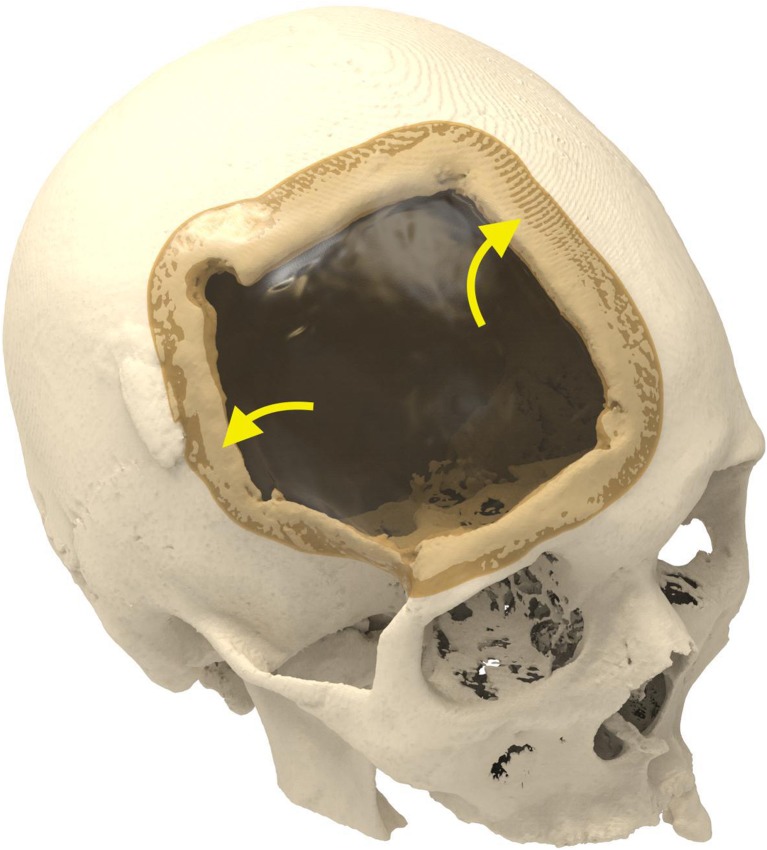
Objective, design, and setting: In an attempt to decrease complications related to polyether-ether-ketone (PEEK) cranioplasty, we gradually made changes to implant design and cranioplasty techniques. These changes include under-contouring of the implant and the use of segmented plates for large defects, microplate fixation for small temporal defects, temporal shell implants to reconstruct the temporalis muscle, and perforations to facilitate the drainage of blood and cerebrospinal fluid and serve as fixation points.
Results: From June 2016 to June 2017, 18 patients underwent cranioplasty, and a total of 31 PEEK and titanium implants were inserted. All implants were successful.
Conclusions: These changes to implant design and cranioplasty techniques facilitate the insertion and fixation of patient-specific cranial implants and improve esthetic outcomes.
Keywords: Computer-aided design; Cranium; Implant.
Conflict of interest statement
Conflict of interest
Erik Nout declares that he has no conflict of interest.
Maurice Mommaerts declares that he is innovation manager at CADskills bvba.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical committee review was deemed not necessary as this is a study on product design not on clinical outcomes.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures


Comment in
-
Letter to the editor: "Considerations in computer-aided design for inlay cranioplasty: technical note".Oral Maxillofac Surg. 2018 Mar;22(1):117-118. doi: 10.1007/s10006-018-0683-0. Epub 2018 Feb 3. Oral Maxillofac Surg. 2018. PMID: 29397448 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
