

Racial, Ethnic, and Gender Equity in Veteran Satisfaction with Health Care in the Veterans Affairs Health Care System
- PMID: 29313226
- PMCID: PMC5834960
- DOI: 10.1007/s11606-017-4221-9
Racial, Ethnic, and Gender Equity in Veteran Satisfaction with Health Care in the Veterans Affairs Health Care System
Abstract
Background: Patient satisfaction is an important dimension of health care quality. The Veterans Health Administration (VA) is committed to providing high-quality care to an increasingly diverse patient population.
Objective: To assess Veteran satisfaction with VA health care by race/ethnicity and gender.
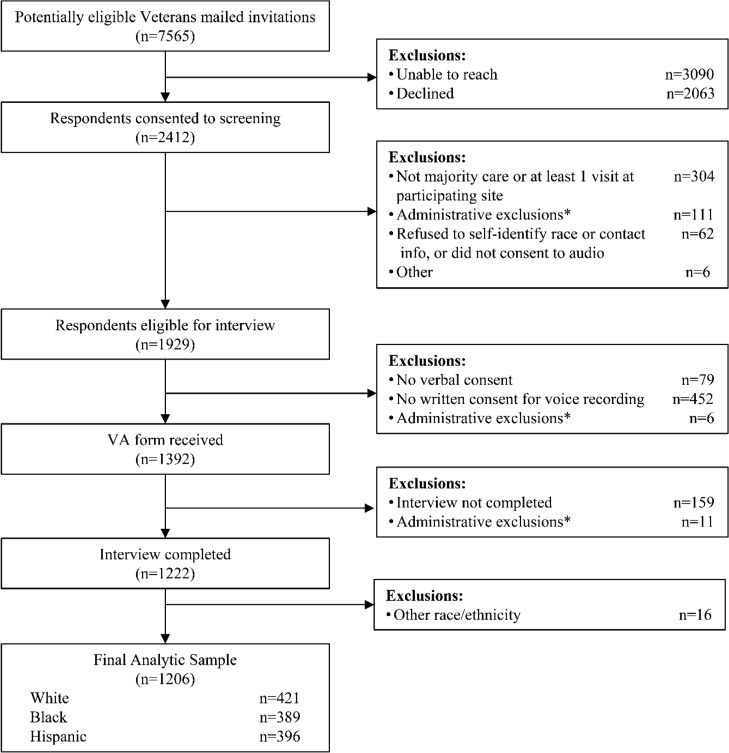
Design and participants: We conducted semi-structured telephone interviews with gender-specific stratified samples of black, white, and Hispanic Veterans from 25 predominantly minority-serving VA Medical Centers from June 2013 to January 2015.
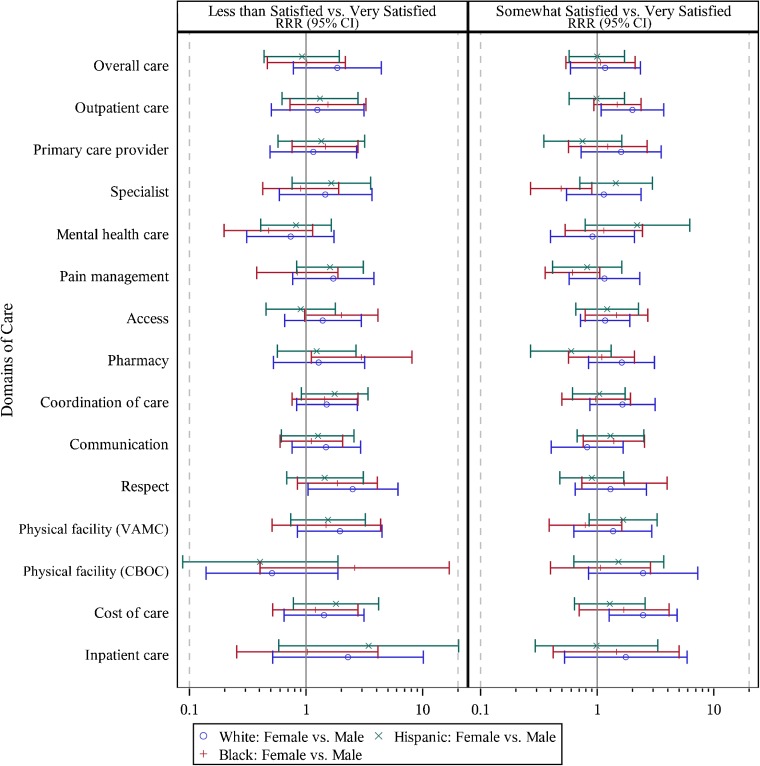
Main measures: Satisfaction with health care was assessed in 16 domains using five-point Likert scales. We compared the proportions of Veterans who were very satisfied, somewhat satisfied, and less than satisfied (i.e., neither satisfied nor dissatisfied, somewhat dissatisfied, or very dissatisfied) in each domain, and used random-effects multinomial regression to estimate racial/ethnic differences by gender and gender differences by race/ethnicity.
Key results: Interviews were completed for 1222 of the 1929 Veterans known to be eligible for the interview (63.3%), including 421 white, 389 black, and 396 Hispanic Veterans, 616 of whom were female. Veterans were less likely to be somewhat satisfied or less than satisfied versus very satisfied with care in each of the 16 domains. The highest satisfaction ratings were reported for costs, outpatient facilities, and pharmacy (74-76% very satisfied); the lowest ratings were reported for access, pain management, and mental health care (21-24% less than satisfied). None of the joint tests of racial/ethnic or gender differences in satisfaction (simultaneously comparing all three satisfaction levels) was statistically significant (p > 0.05). Pairwise comparisons of specific levels of satisfaction revealed racial/ethnic differences by gender in three domains and gender differences by race/ethnicity in five domains, with no consistent directionality across demographic subgroups.
Conclusions: Our multisite interviews of a diverse sample of Veterans at primarily minority-serving sites showed generally high levels of health care satisfaction across 16 domains, with few quantitative differences by race/ethnicity or gender.
Keywords: health care disparities; patient satisfaction; veterans.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures




Comment in
-
Capsule Commentary on Zickmund et al., Racial, Ethnic, and Gender Equity in Veteran Satisfaction with Health Care in the Veterans Affairs Health Care System.J Gen Intern Med. 2018 Mar;33(3):333. doi: 10.1007/s11606-017-4253-1. J Gen Intern Med. 2018. PMID: 29256087 Free PMC article. No abstract available.
References
-
- Institute of Medicine Committee on Quality of Health Care in America . Crossing the quality chasm: A new health system for the 21st century. Washington (DC): National Academies Press; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
