

Retinoblastoma, the visible CNS tumor: A review
- PMID: 29314142
- PMCID: PMC6034991
- DOI: 10.1002/jnr.24213
Retinoblastoma, the visible CNS tumor: A review
Abstract
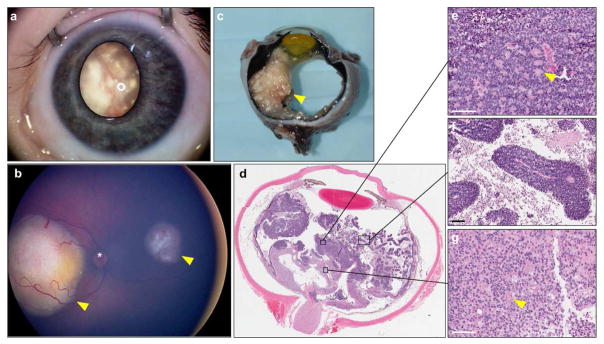
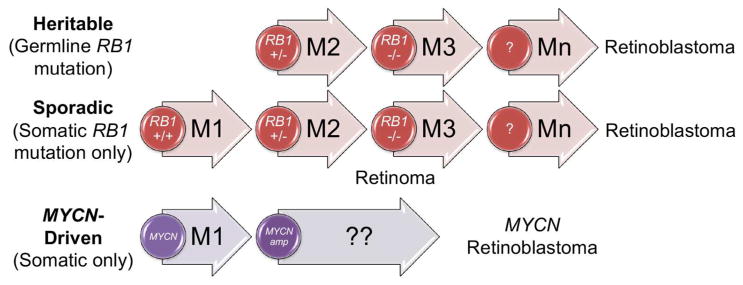
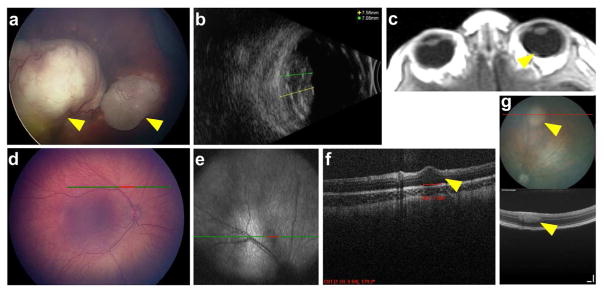
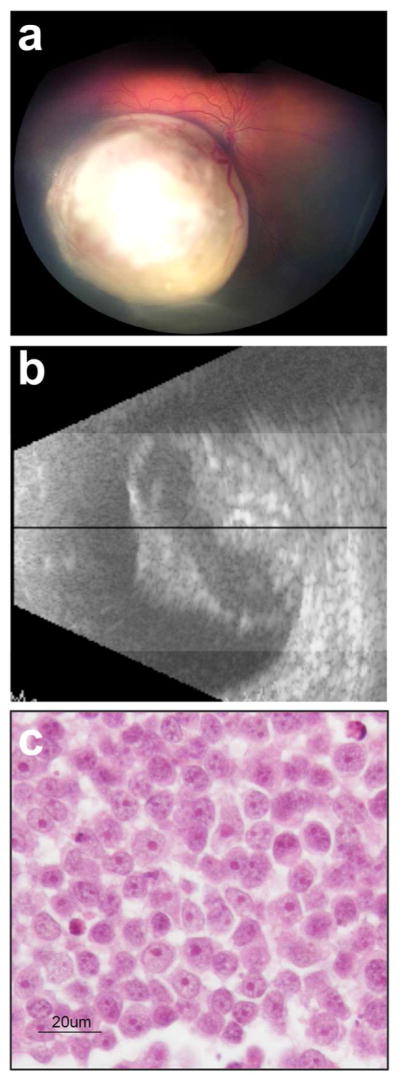
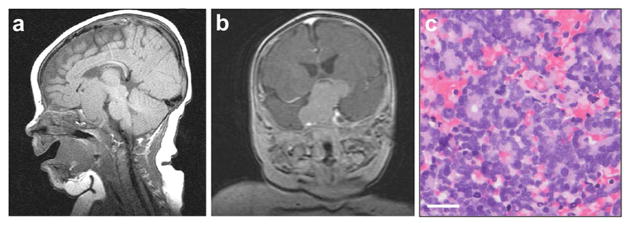
The pediatric ocular cancer retinoblastoma is the only central nervous system (CNS) tumor readily observed without specialized equipment: it can be seen by, and in, the naked eye. This accessibility enables unique imaging modalities. Here, we review this cancer for a neuroscience audience, highlighting these clinical and research imaging options, including fundus imaging, optical coherence tomography, ultrasound, and magnetic resonance imaging. We also discuss the subtype of retinoblastoma driven by the MYCN oncogene more commonly associated with neuroblastoma, and consider trilateral retinoblastoma, in which an intracranial tumor arises along with ocular tumors in patients with germline RB1 gene mutations. Retinoblastoma research and clinical care can offer insights applicable to CNS malignancies, and also benefit from approaches developed elsewhere in the CNS.
Keywords: MYCN; cancer genetics; neuroimaging; optical coherence tomography; pediatric cancer; pineoblastoma.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Bader JL, Miller RW, Meadows AT, Zimmerman LE, Champion LA, Voute PA. Trilateral retinoblastoma. Lancet. 1980;2(8194):582–583. - PubMed
-
- Bastawrous A. Increasing access to eye care ... there’s an app for that. Peek: smartphone technology for eye health. Int J Epidemiol. 2016;45(4):1040–1043. - PubMed
-
- Beck Popovic M, Balmer A, Maeder P, Braganca T, Munier FL. Benign pineal cysts in children with bilateral retinoblastoma: a new variant of trilateral retinoblastoma? Pediatr Blood Cancer. 2006;46(7):755–761. - PubMed
-
- Benavente CA, Dyer MA. Genetics and epigenetics of human retinoblastoma. Annu Rev Pathol. 2015;10:547–562. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
