

Factors Influencing Time-to-diagnosis of Biliary Atresia
- PMID: 29315162
- PMCID: PMC5963977
- DOI: 10.1097/MPG.0000000000001887
Factors Influencing Time-to-diagnosis of Biliary Atresia
Abstract
Objectives: Diagnosing biliary atresia (BA) quickly is critical, because earlier treatment correlates with delayed or reduced need for liver transplantation. However, diagnosing BA quickly is also difficult, with infants usually treated after 60 days of life. In this study, we aim to accelerate BA diagnosis and treatment, by better understanding factors influencing the diagnostic timeline.
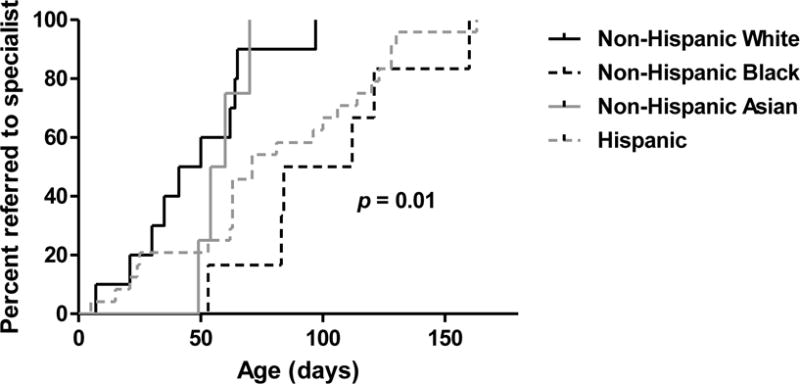
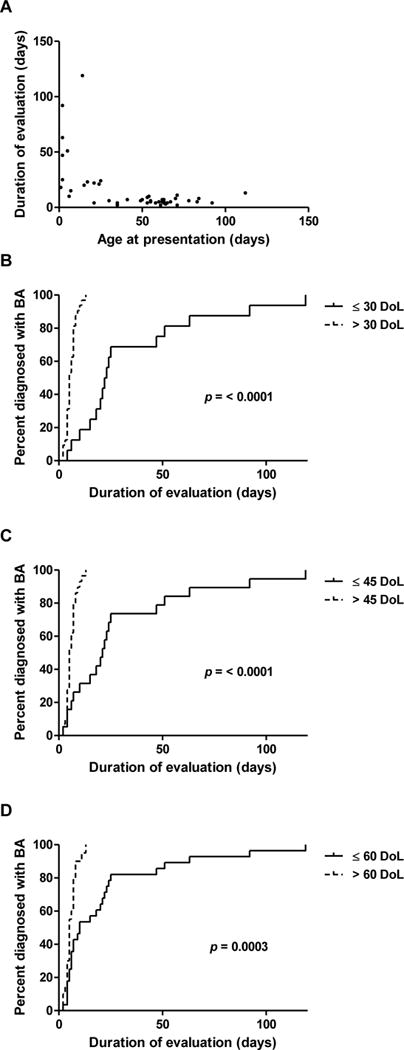
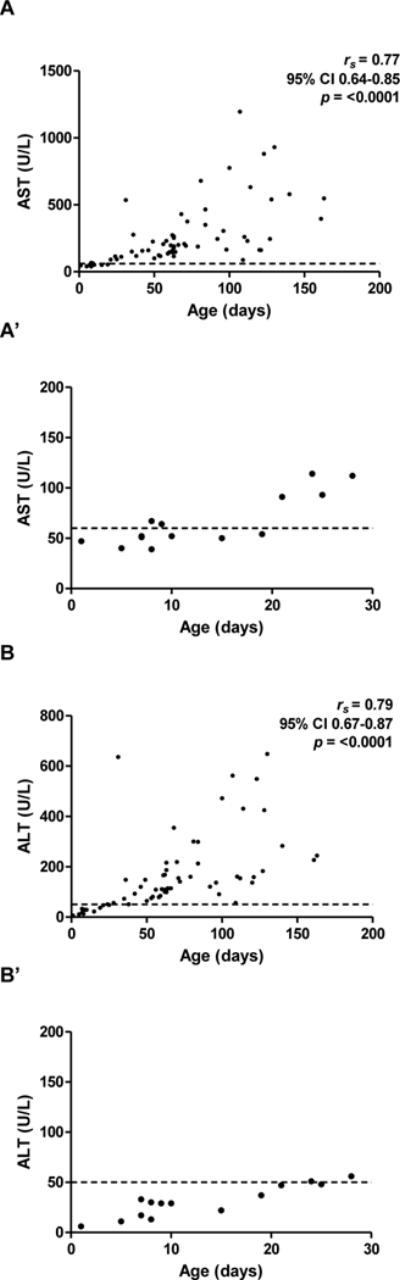
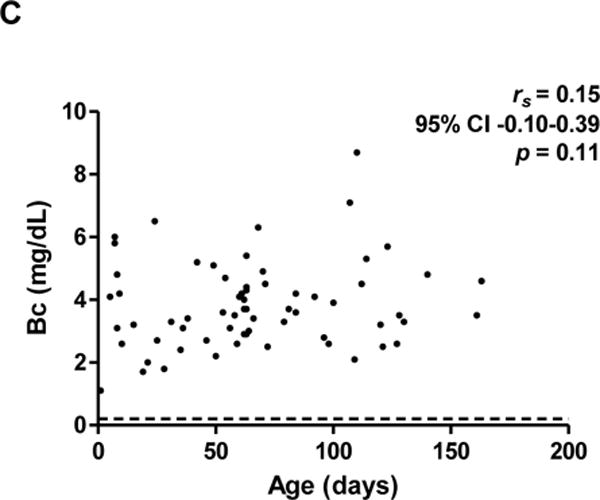
Methods: Infants born between 2007 and 2014 and diagnosed with BA at our institution were included (n = 65). Two periods were examined retrospectively: P1, the time from birth to specialist referral, and P2, the time from specialist referral to treatment. How sociodemographic factors associate with P1 and P2 were analyzed with Kaplan-Meier curves and Cox proportional hazard models. In addition, to better characterize P2, laboratory results and early tissue histology were studied.
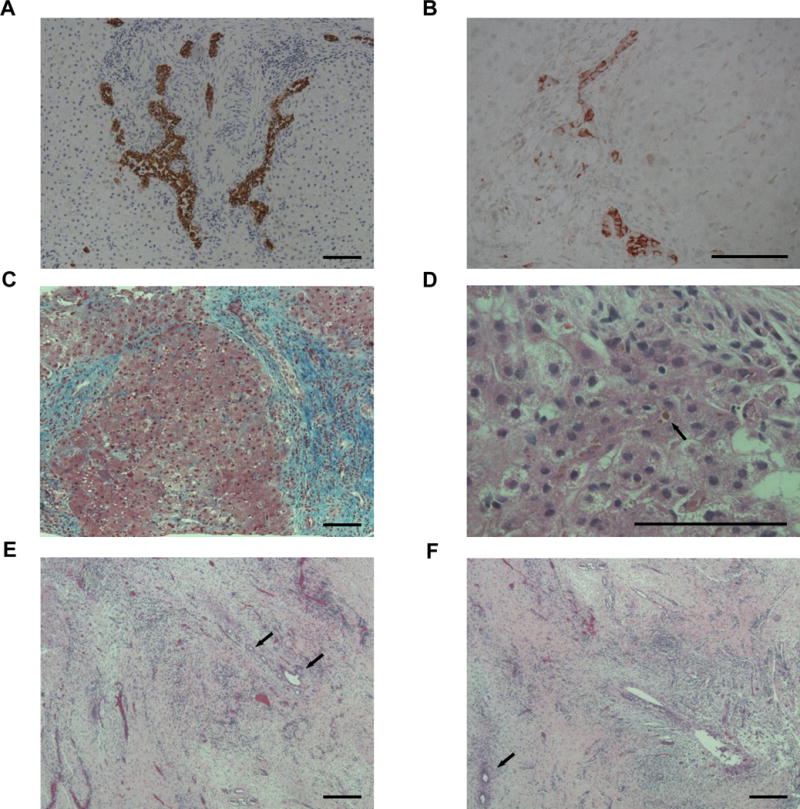
Results: P1 associated with race/ethnicity, with shorter times in non-Hispanic white infants compared to non-Hispanic black and Hispanic infants (P = 0.007 and P = 0.004, respectively). P2 associated with referral age, with shorter times in infants referred after 30, 45, or 60 days of life (P < 0.001, P < 0.001, and P = 0.001, respectively). One potential reason for longer P2 in infants referred ≤30 days is that aminotransferase levels were normal or near-normal. However, despite reassuring laboratory values, tissue histology in early cases showed key features of BA.
Conclusions: Our findings suggest 2 opportunities to accelerate BA diagnosis and treatment. First, to achieve prompt referrals for all races/ethnicities, universal screening strategies should be considered. Second, to ensure efficient evaluations independent of age, algorithms designed to detect early features of BA can be developed.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
