

Novel Methods for Reporting of Exercise Dose and Adherence: An Exploratory Analysis
- PMID: 29315168
- PMCID: PMC5953772
- DOI: 10.1249/MSS.0000000000001545
Novel Methods for Reporting of Exercise Dose and Adherence: An Exploratory Analysis
Abstract
Purpose: The purpose of this study was to explore whether methods adapted from oncology pharmacological trials have utility in reporting adherence (tolerability) of exercise treatment in cancer.
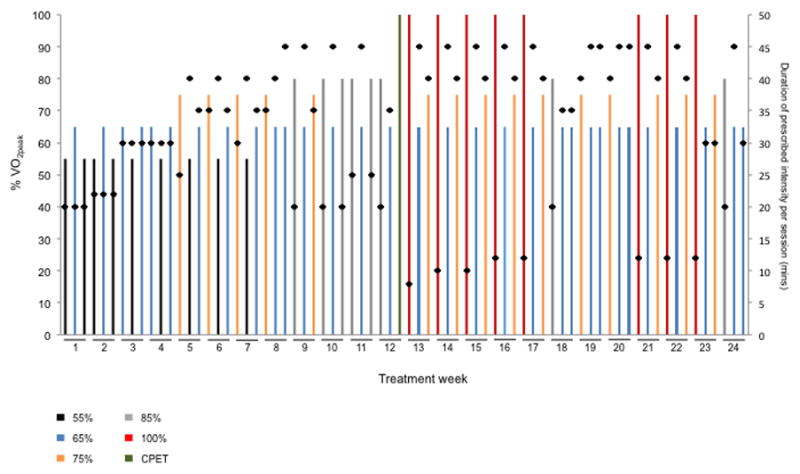
Methods: Using a retrospective analysis of a randomized trial, 25 prostate cancer patients received an aerobic training regimen of 72 supervised treadmill walking sessions delivered thrice weekly between 55% and 100% of exercise capacity for 24 consecutive weeks. Treatment adherence (tolerability) was assessed using conventional (lost to follow-up and attendance) and exploratory (e.g., permanent discontinuation, dose modification, and relative dose intensity) outcomes.
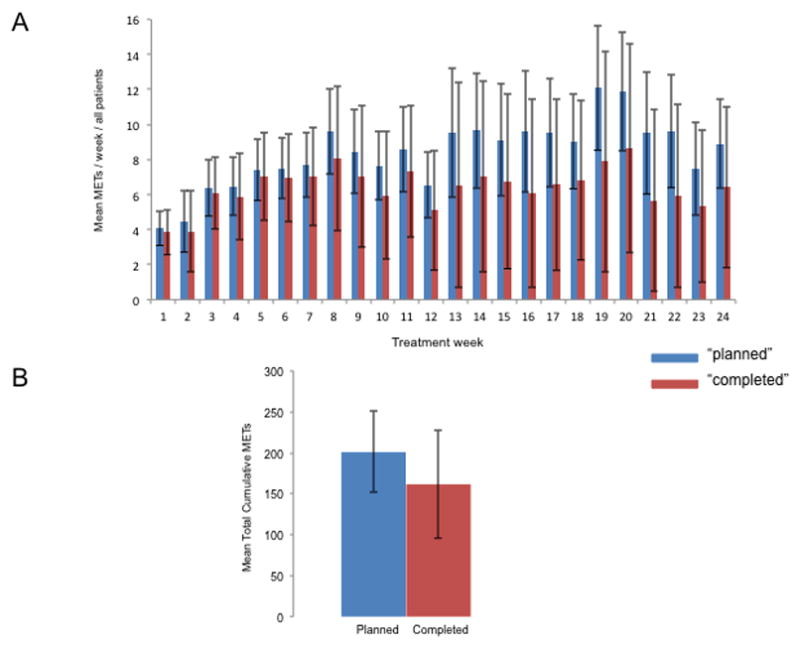
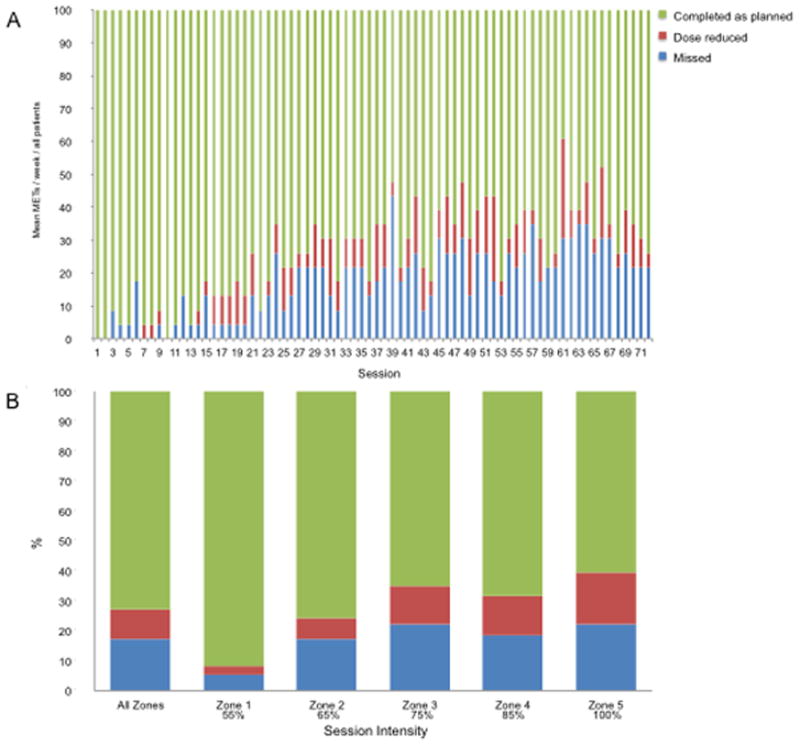
Results: The mean total cumulative "planned" and "completed" dose was 200.7 ± 47.6 and 153.8 ± 68.8 MET·h, respectively, equating to a mean relative dose intensity of 77% ± 24%. Two patients (8%) were lost to follow-up, and mean attendance was 79%. A total of 6 (24%) of 25 patients permanently discontinued aerobic training before week 24. Aerobic training was interrupted (missing ≥3 consecutive sessions) or dose reduced in a total of 11 (44%) and 24 (96%) patients, respectively; a total 185 (10%) of 1800 training sessions required dose reduction owing to both health-related (all nonserious) and non-health-related adverse events. Eighteen (72%) patients required at least one session to be terminated early; a total of 59 (3%) sessions required early termination.
Conclusions: Novel methods for the conduct and reporting of exercise treatment adherence and tolerability may provide important information beyond conventional metrics in patients with cancer.
Figures
References
-
- Schmitz KH, Ahmed RL, Troxel A, et al. Weight lifting in women with breast-cancer-related lymphedema. The New England journal of medicine. 2009;361(7):664–73. - PubMed
-
- Courneya KS, Sellar CM, Stevinson C, et al. Randomized controlled trial of the effects of aerobic exercise on physical functioning and quality of life in lymphoma patients. J Clin Oncol. 2009;27(27):4605–12. - PubMed
-
- Segal RJ, Reid RD, Courneya KS, et al. Randomized controlled trial of resistance or aerobic exercise in men receiving radiation therapy for prostate cancer. J Clin Oncol. 2009;27(3):344–51. - PubMed
-
- Galvao DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol. 2010;28(2):340–7. - PubMed
-
- Courneya KS, Mackey JR, Bell GJ, Jones LW, Field CJ, Fairey AS. Randomized controlled trial of exercise training in postmenopausal breast cancer survivors: cardiopulmonary and quality of life outcomes. J Clin Oncol. 2003;21(9):1660–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
