

Cerebrovascular Events in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
- PMID: 29316357
- PMCID: PMC6033693
- DOI: 10.1002/acr.23509
Cerebrovascular Events in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
Abstract
Objective: To determine the frequency, characteristics, and outcomes of cerebrovascular events (CerVEs), as well as clinical and autoantibody associations in a multiethnic/racial inception cohort of patients with systemic lupus erythematosus (SLE).
Methods: A total of 1,826 patients were assessed annually for 19 neuropsychiatric (NP) events, including 5 types of CerVEs: 1) stroke, 2) transient ischemia, 3) chronic multifocal ischemia, 4) subarachnoid/intracranial hemorrhage, and 5) sinus thrombosis. Global disease activity (Systemic Lupus Erythematosus Disease [SLE] Activity Index 2000), damage scores (SLE International Collaborating Clinics/American College of Rheumatology Damage Index), and Short Form 36 (SF-36) scores were collected. Time to event, linear and logistic regressions, and multistate models were used as appropriate.
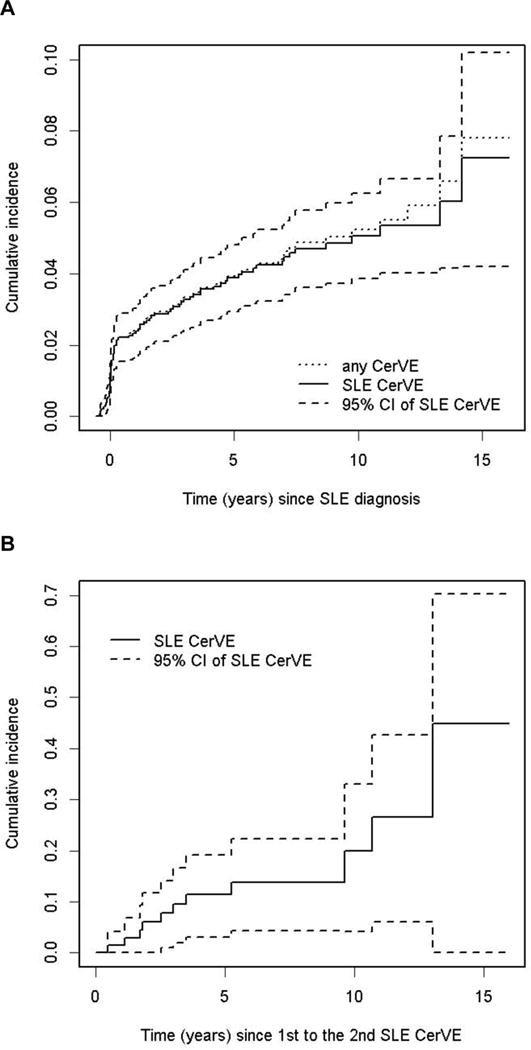
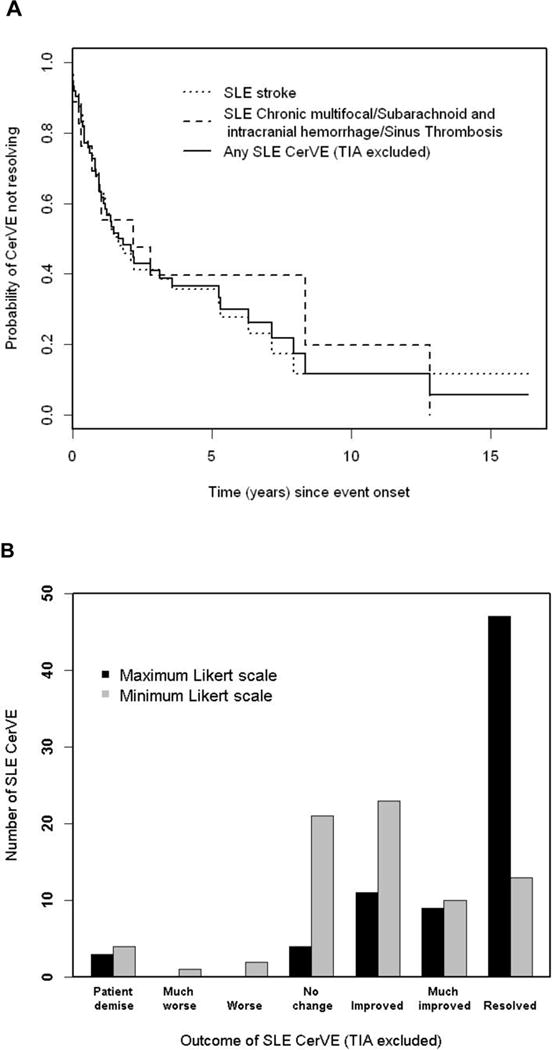
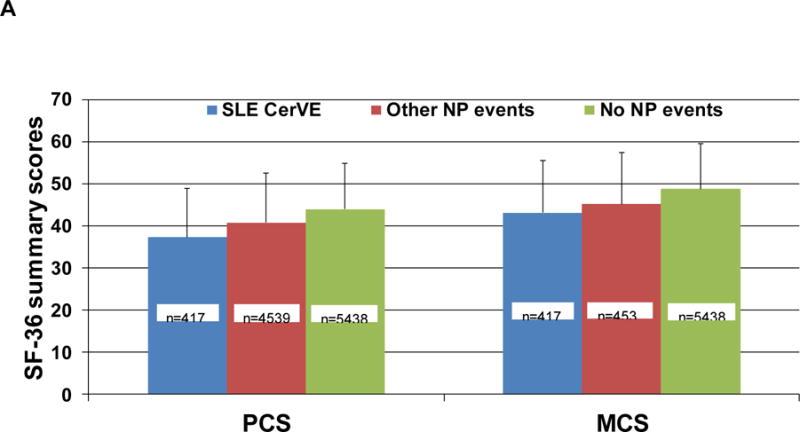
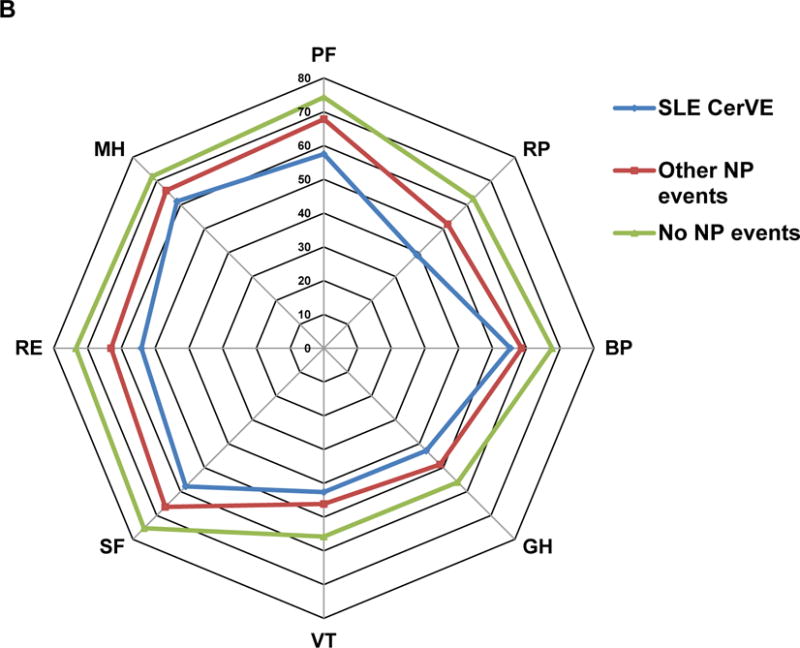
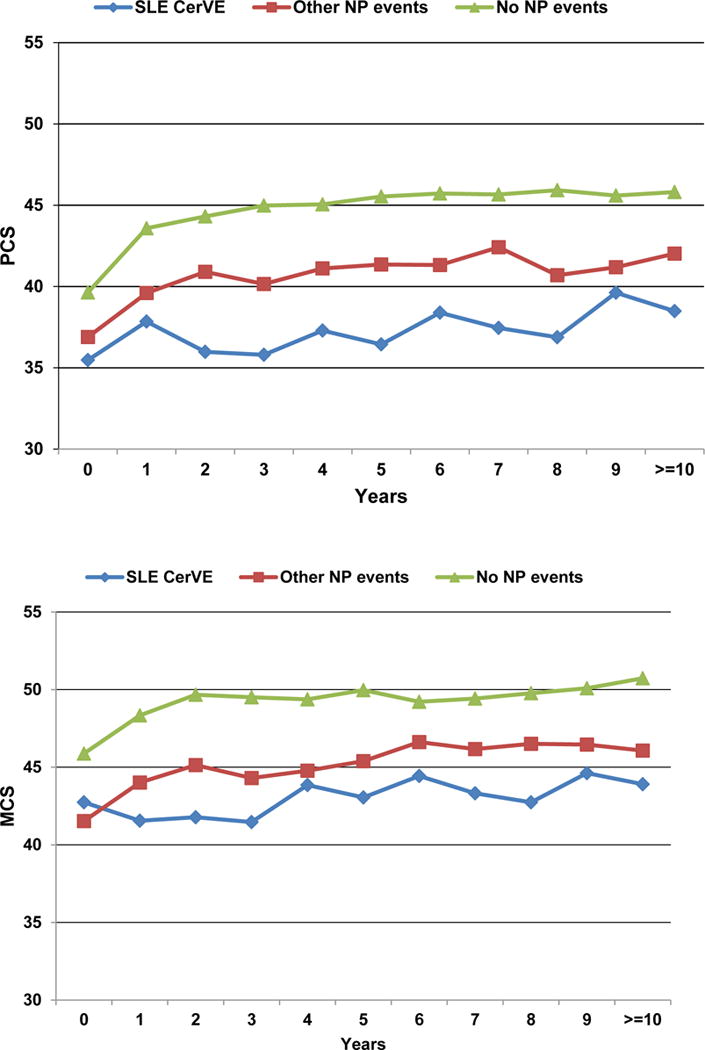
Results: CerVEs were the fourth most frequent NP event: 82 of 1,826 patients had 109 events; of these events, 103 were attributed to SLE, and 44 were identified at the time of enrollment. The predominant events were stroke (60 of 109 patients) and transient ischemia (28 of 109 patients). CerVEs were associated with other NP events attributed to SLE, non-SLE-attributed NP events, African ancestry (at US SLICC sites), and increased organ damage scores. Lupus anticoagulant increased the risk of first stroke and sinus thrombosis and transient ischemic attack. Physician assessment indicated resolution or improvement in the majority of patients, but patients reported sustained reduction in SF-36 summary and subscale scores following a CerVE.
Conclusion: CerVEs, the fourth most frequent NP event in SLE, are usually attributable to lupus. In contrast to good physician-reported outcomes, patients reported a sustained reduction in health-related quality of life following a CerVE.
© 2018, American College of Rheumatology.
Figures
References
-
- Ainiala H, Loukkola J, Peltola J, Korpela M, Hietaharju A. The prevalence of neuropsychiatric syndromes in systemic lupus erythematosus. Neurology. 2001;57:496–500. - PubMed
-
- Brey RL, Holliday SL, Saklad AR, et al. Neuropsychiatric syndromes in lupus: prevalence using standardized definitions. Neurology. 2002;58:1214–20. - PubMed
-
- Hanly JG, McCurdy G, Fougere L, Douglas JA, Thompson K. Neuropsychiatric events in systemic lupus erythematosus: attribution and clinical significance. J Rheumatol. 2004;31:2156–62. - PubMed
-
- Sanna G, Bertolaccini ML, Cuadrado MJ, Laing H, Mathieu A, Hughes GR. Neuropsychiatric manifestations in systemic lupus erythematosus: prevalence and association with antiphospholipid antibodies. J Rheumatol. 2003;30:985–92. - PubMed
-
- Sibbitt WL, Jr, Brandt JR, Johnson CR, et al. The incidence and prevalence of neuropsychiatric syndromes in pediatric onset systemic lupus erythematosus. J Rheumatol. 2002;29:1536–42. - PubMed
Publication types
MeSH terms
Grants and funding
- AR-69572/AR/NIAMS NIH HHS/United States
- M01 RR000046/RR/NCRR NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- 5-UL-1TR001422-02/TR/NCATS NIH HHS/United States
- P60-AR-64464/AR/NIAMS NIH HHS/United States
- DH_/Department of Health/United Kingdom
- UL1 RR025741/RR/NCRR NIH HHS/United States
- AR-43727/AR/NIAMS NIH HHS/United States
- P30 AR072579/AR/NIAMS NIH HHS/United States
- RR-00046/RR/NCRR NIH HHS/United States
- MC_UU_00002/8/MRC_/Medical Research Council/United Kingdom
- MC_U105261167/MRC_/Medical Research Council/United Kingdom
- P60-AR-48098/AR/NIAMS NIH HHS/United States
- P60 AR064464/AR/NIAMS NIH HHS/United States
- P60 AR048098/AR/NIAMS NIH HHS/United States
- U105261167/MRC_/Medical Research Council/United Kingdom
- UL1 TR001422/TR/NCATS NIH HHS/United States
- MOP-88526/CIHR/Canada
- K24-AR-02318/AR/NIAMS NIH HHS/United States
- R01 AR043727/AR/NIAMS NIH HHS/United States
- ARC_/Arthritis Research UK/United Kingdom
- K24 AR002138/AR/NIAMS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- R01 AR069572/AR/NIAMS NIH HHS/United States
- 8-UL-1TR-000150/TR/NCATS NIH HHS/United States
- UL-1RR-025741/RR/NCRR NIH HHS/United States
- MC_UU_00002/3/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
