

Plasma long non-coding RNA BACE1 as a novel biomarker for diagnosis of Alzheimer disease
- PMID: 29316899
- PMCID: PMC5761117
- DOI: 10.1186/s12883-017-1008-x
Plasma long non-coding RNA BACE1 as a novel biomarker for diagnosis of Alzheimer disease
Abstract
Backgrounds: Long non-coding RNA (LncRNA) have been reported to be involved in the pathogenesis of neurodegenerative diseases, but whether it can serve as a biomarker for Alzheimer disease (AD) is not yet known.
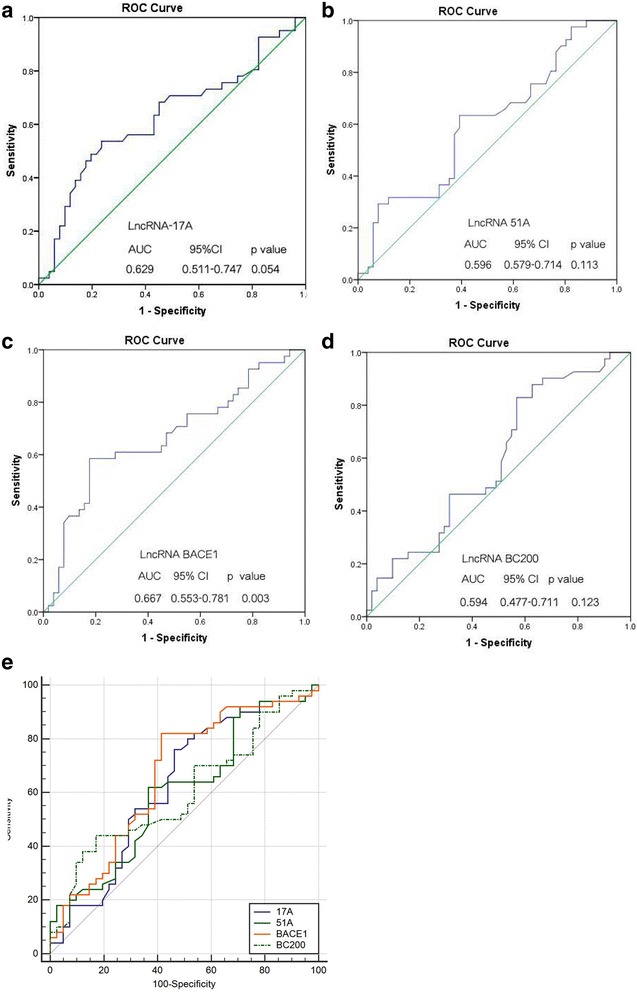
Methods: The present study selected four specific LncRNA (17A, 51A, BACE1 and BC200) as possible AD biomarker. RT-qPCR was performed to validate the LncRNA. Receiver operating characteristic curve (ROC) and area under the ROC curve (AUC) were applied to study the potential of LncRNA as a biomarker in a population of 88 AD patients and 72 control individuals.
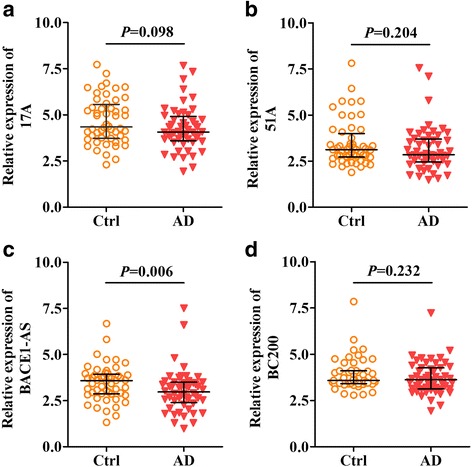
Results: We found that the plasma LncRNA BACE1 level of AD patients was significantly higher than that of healthy controls (p = 0.006). Plasma level of LncRNA 17A, 51A and BC200 did not show a significant difference between two groups (p = 0.098, p = 0.204 and p = 0.232, respectively). ROC curve analysis showed that LncRNA BACE1 was the best candidate of these LncRNA (95% CI: 0.553-0.781, p = 0.003). In addition, no correlation was found for expression of these LncRNA in both control and AD groups with age or MMSE scale (p > 0.05).
Conclusions: Our present study compared the plasma level of four LncRNA between AD and non-AD patients, and found that the level of the BACE1 is increased in the plasma of AD patients and have a high specificity (88%) for AD, indicating BACE1 may be a potential candidate biomarker to predict AD.
Keywords: Alzheimer disease; Biomarker; Diagnosis; Long non-coding RNA.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. In addition, written informed consent was obtained from all patients or their families in accordance with the Declaration of Helsinki.
Consent for publication
Written informed consent for participation and publication was obtained by every participant.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M, Hall K, Hasegawa K, Hendrie H, Huang Y, Jorm A, Mathers C, Menezes PR, Rimmer E, Scazufca M. Alzheimer's disease international. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366:2112–2117. doi: 10.1016/S0140-6736(05)67889-0. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
