

Newer Technologies in Breast Cancer Imaging: Dedicated Cone-Beam Breast Computed Tomography
- PMID: 29317032
- PMCID: PMC5957539
- DOI: 10.1053/j.sult.2017.09.001
Newer Technologies in Breast Cancer Imaging: Dedicated Cone-Beam Breast Computed Tomography
Abstract
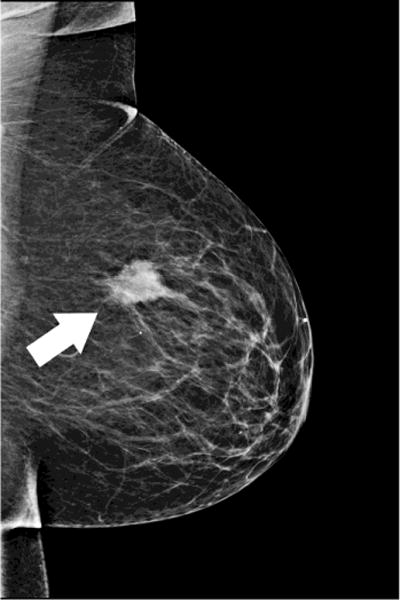
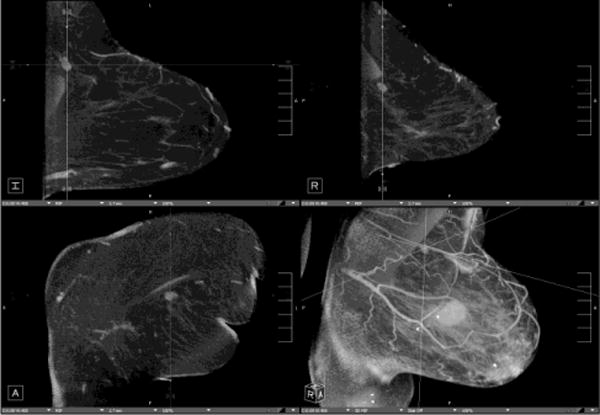
Dedicated breast computed tomography (CT) is the latest in a long history of breast imaging techniques dating back to the 1960s. Breast imaging is performed both for cancer screening as well as for diagnostic evaluation of symptomatic patients. Dedicated breast CT received US Food and Drug Administration approval for diagnostic use in 2015 and is slowly gaining recognition for its value in diagnostic 3-dimensional imaging of the breast, and also for injected contrast-enhanced imaging applications. Conventional mammography has known limitations in sensitivity and specificity, especially in dense breasts. Breast tomosynthesis was US Food and Drug Administration approved in 2011 and is now widely used. Dedicated breast CT is the next technological advance, combining real 3-dimensional imaging with the ease of contrast administration. The lack of painful compression and manipulation of the breasts also makes dedicated breast CT much more acceptable for the patients.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures










References
-
- Chang CH, Sibala JL, Fritz SL, Dwyer SJ, 3rd, Templeton AW, Lin F, et al. Computed tomography in detection and diagnosis of breast cancer. Cancer. 1980;46(4 Suppl):939–46. - PubMed
-
- Raptopoulos V, Baum JK, Hochman M, Karellas A, Houlihan MJ, D’Orsi CJ. High resolution CT mammography of surgical biopsy specimens. J Comput Assist Tomogr. 1996;20(2):179–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
