

Association of Screening and Treatment With Breast Cancer Mortality by Molecular Subtype in US Women, 2000-2012
- PMID: 29318276
- PMCID: PMC5833658
- DOI: 10.1001/jama.2017.19130
Association of Screening and Treatment With Breast Cancer Mortality by Molecular Subtype in US Women, 2000-2012
Erratum in
-
Error in Figure.JAMA. 2018 Feb 20;319(7):724. doi: 10.1001/jama.2018.0632. JAMA. 2018. PMID: 29466570 Free PMC article. No abstract available.
Abstract
Importance: Given recent advances in screening mammography and adjuvant therapy (treatment), quantifying their separate and combined effects on US breast cancer mortality reductions by molecular subtype could guide future decisions to reduce disease burden.
Objective: To evaluate the contributions associated with screening and treatment to breast cancer mortality reductions by molecular subtype based on estrogen-receptor (ER) and human epidermal growth factor receptor 2 (ERBB2, formerly HER2 or HER2/neu).
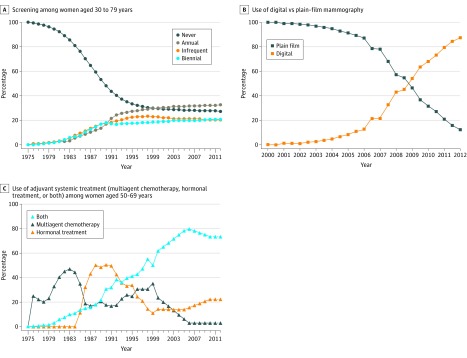
Design, setting, and participants: Six Cancer Intervention and Surveillance Network (CISNET) models simulated US breast cancer mortality from 2000 to 2012 using national data on plain-film and digital mammography patterns and performance, dissemination and efficacy of ER/ERBB2-specific treatment, and competing mortality. Multiple US birth cohorts were simulated.
Exposures: Screening mammography and treatment.
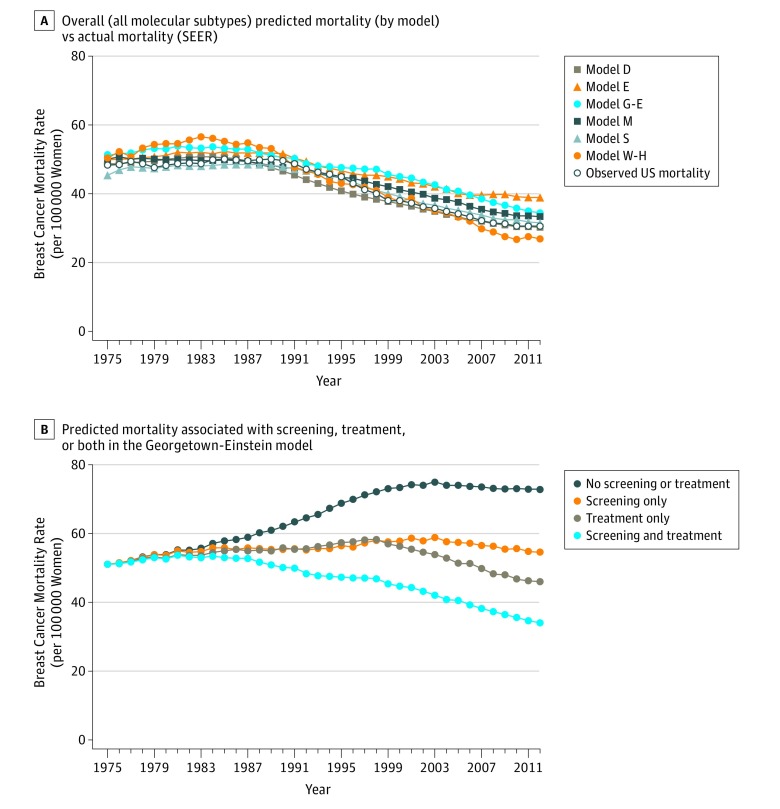
Main outcomes and measures: The models compared age-adjusted, overall, and ER/ERBB2-specific breast cancer mortality rates from 2000 to 2012 for women aged 30 to 79 years relative to the estimated mortality rate in the absence of screening and treatment (baseline rate); mortality reductions were apportioned to screening and treatment.
Results: In 2000, the estimated reduction in overall breast cancer mortality rate was 37% (model range, 27%-42%) relative to the estimated baseline rate in 2000 of 64 deaths (model range, 56-73) per 100 000 women: 44% (model range, 35%-60%) of this reduction was associated with screening and 56% (model range, 40%-65%) with treatment. In 2012, the estimated reduction in overall breast cancer mortality rate was 49% (model range, 39%-58%) relative to the estimated baseline rate in 2012 of 63 deaths (model range, 54-73) per 100 000 women: 37% (model range, 26%-51%) of this reduction was associated with screening and 63% (model range, 49%-74%) with treatment. Of the 63% associated with treatment, 31% (model range, 22%-37%) was associated with chemotherapy, 27% (model range, 18%-36%) with hormone therapy, and 4% (model range, 1%-6%) with trastuzumab. The estimated relative contributions associated with screening vs treatment varied by molecular subtype: for ER+/ERBB2-, 36% (model range, 24%-50%) vs 64% (model range, 50%-76%); for ER+/ERBB2+, 31% (model range, 23%-41%) vs 69% (model range, 59%-77%); for ER-/ERBB2+, 40% (model range, 34%-47%) vs 60% (model range, 53%-66%); and for ER-/ERBB2-, 48% (model range, 38%-57%) vs 52% (model range, 44%-62%).
Conclusions and relevance: In this simulation modeling study that projected trends in breast cancer mortality rates among US women, decreases in overall breast cancer mortality from 2000 to 2012 were associated with advances in screening and in adjuvant therapy, although the associations varied by breast cancer molecular subtype.
Conflict of interest statement
Figures
Comment in
-
Contributions of Screening and Treatment to Mortality From Breast Cancer.JAMA. 2018 Jun 12;319(22):2335-2336. doi: 10.1001/jama.2018.4238. JAMA. 2018. PMID: 29896620 No abstract available.
References
-
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Breast Cancer Statistics. https://seer.cancer.gov/statfacts/html/breast.html. Accessed March 31, 2017.
-
- Berry DA, Cronin KA, Plevritis SK, et al. ; Cancer Intervention and Surveillance Modeling Network (CISNET) Collaborators . Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353(17):1784-1792. - PubMed
-
- Giordano SH, Temin S, Kirshner JJ, et al. ; American Society of Clinical Oncology . Systemic therapy for patients with advanced human epidermal growth factor receptor 2-positive breast cancer: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2014;32(19):2078-2099. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
