

New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation
- PMID: 29318587
- PMCID: PMC6057895
- DOI: 10.1111/bph.14116
New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation
Abstract
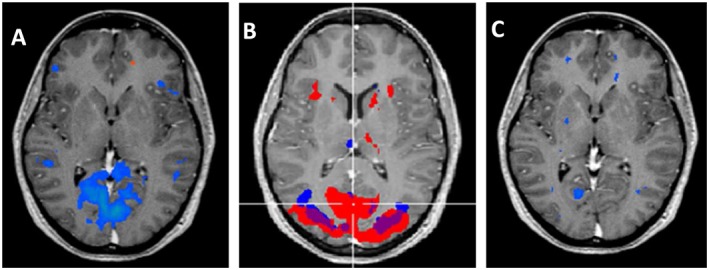
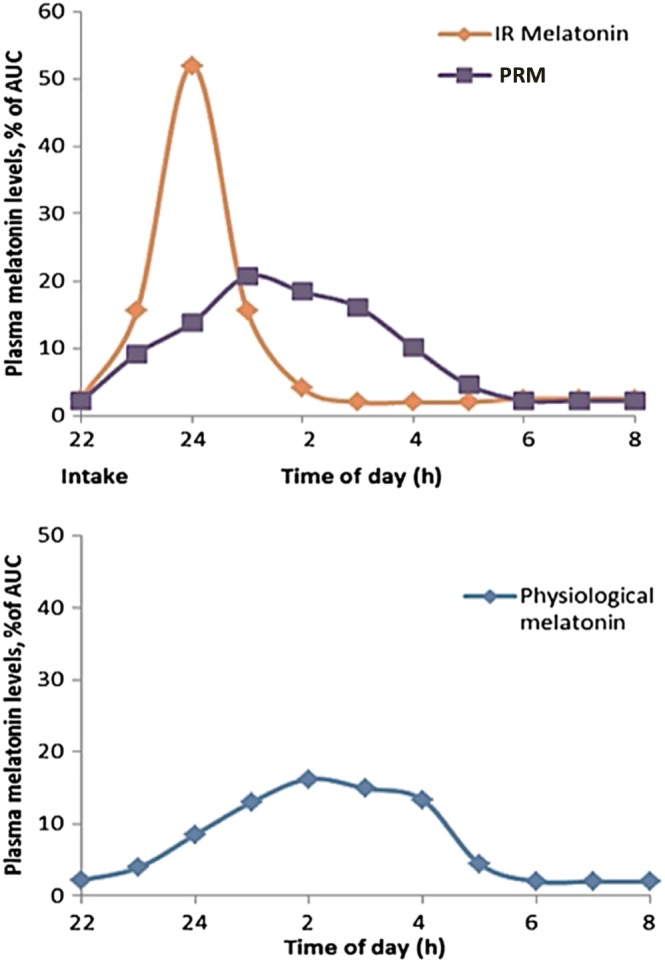
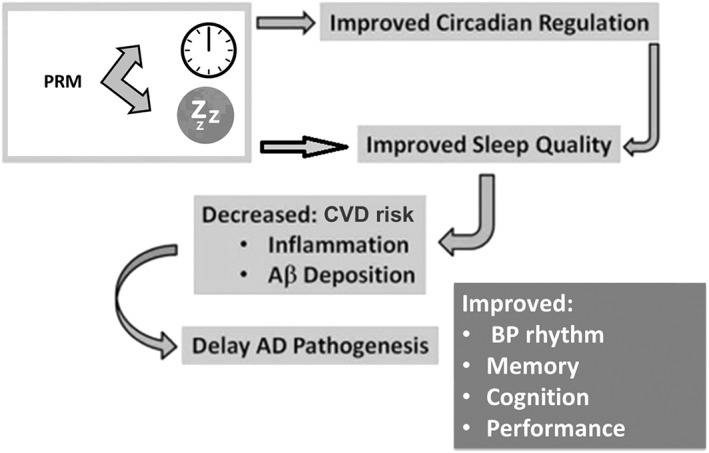
In mammals, a central circadian clock, located in the suprachiasmatic nuclei (SCN) of the hypothalamus, tunes the innate circadian physiological rhythms to the ambient 24 h light-dark cycle to invigorate and optimize the internal temporal order. The SCN-activated, light-inhibited production of melatonin conveys the message of darkness to the clock and induces night-state physiological functions, for example, sleep/wake blood pressure and metabolism. Clinically meaningful effects of melatonin treatment have been demonstrated in placebo-controlled trials in humans, particularly in disorders associated with diminished or misaligned melatonin rhythms, for example, circadian rhythm-related sleep disorders, jet lag and shift work, insomnia in children with neurodevelopmental disorders, poor (non-restorative) sleep quality, non-dipping nocturnal blood pressure (nocturnal hypertension) and Alzheimer's disease (AD). The diminished production of melatonin at the very early stages of AD, the role of melatonin in the restorative value of sleep (perceived sleep quality) and its sleep-anticipating effects resulting in attenuated activation of certain brain networks are gaining a new perspective as the role of poor sleep quality in the build-up of β amyloid, particularly in the precuneus, is unravelled. As a result of the recently discovered relationship between circadian clock, sleep and neurodegeneration, new prospects of using melatonin for early intervention, to promote healthy physical and mental ageing, are of prime interest in view of the emerging link to the aetiology of Alzheimer's disease. LINKED ARTICLES: This article is part of a themed section on Recent Developments in Research of Melatonin and its Potential Therapeutic Applications. To view the other articles in this section visit http://onlinelibrary.wiley.com/doi/10.1111/bph.v175.16/issuetoc.
© 2018 The Authors. British Journal of Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Figures
References
-
- APA (2008). Primary insomnia In: Diagnostic and Statistical Manual of Mental Disorders. Americal Psychiatric Association: Washington, DC.
-
- Arbon EL, Knurowska M, Dijk DJ (2015). Randomised clinical trial of the effects of prolonged‐release melatonin, temazepam and zolpidem on slow‐wave activity during sleep in healthy people. J Psychopharmacol 29: 764–776. - PubMed
-
- Brugger P, Marktl W, Herold M (1995). Impaired nocturnal secretion of melatonin in coronary heart disease. Lancet 345: 1408. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
