

Review
doi: 10.1056/NEJMra1401483.
Multiple Sclerosis
Affiliations
- PMID: 29320652
- PMCID: PMC6942519
- DOI: 10.1056/NEJMra1401483
Item in Clipboard
Review
Multiple Sclerosis
N Engl J Med.
.
No abstract available
Figures
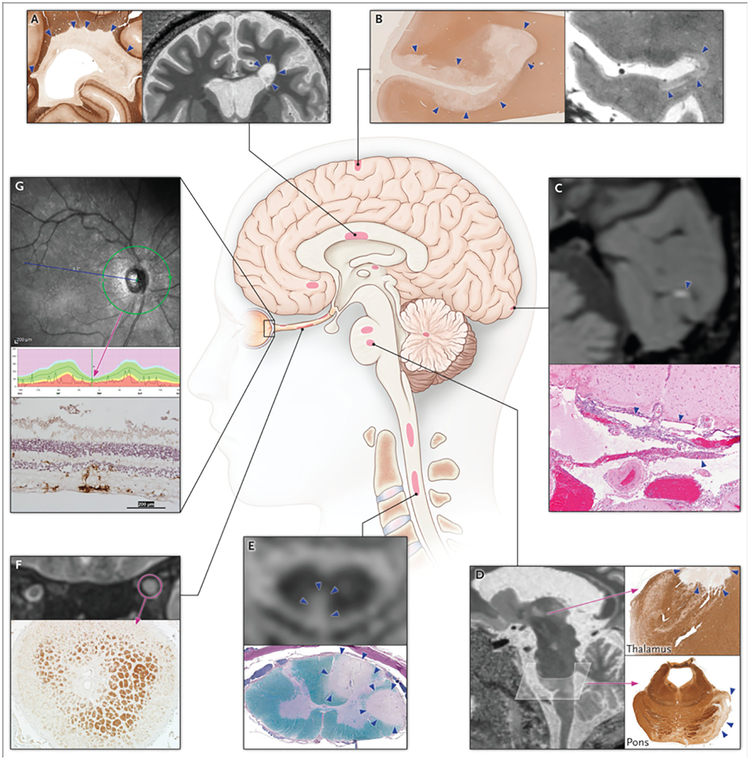
Schematic of lesion location, calling out imaging and pathological examples, in the (A) periventricular white matter; (B) subpial cortex; (C) leptomeninges; (D) thalamus and pons; (E) spinal cord; (F) optic nerve; and (G) retina. (A, B, D) 7-tesla MRI of a 40-year-old woman with relapsing-remitting MS, with similar pathological findings (in different cases) highlighted by immunohistochemistry directed against myelin proteolipid protein. (C) 3-tesla post-gadolinium MRI of a 35-year-old woman with secondary progressive MS, with corresponding pathological findings in the meninges of a different case (hematoxylin and eosin stain). (E) 3-tesla MRI of a 60-year-old woman with relapsing-remitting MS and corresponding pathological findings in a different case (Luxol fast blue-periodic acid Schiff stain). (F) 3-tesla MRI of a 31-year-old woman with relapsing-remitting MS and corresponding pathological findings in a different case (anti-proteolipid protein immunohistochemistry). (G) Spectral-domain optical coherence tomography reconstruction showing thinning of the peripapillary retinal nerve fiber layer. The normal range of retinal thickness is shown in green, and for this particular individual (black line) the retina is thinner than 99% of control eyes. The bottom panel shows corresponding pathological findings in a different case (immunohistochemistry for Iba-1, a microglial marker, with hematoxylin counterstain). Lesions are denoted with arrows or circles.
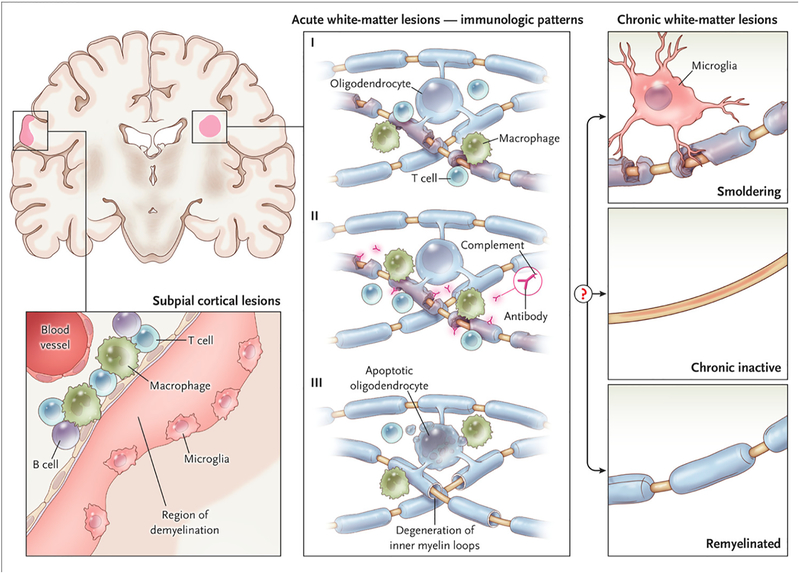
Early active white matter demyelination falls into three major categories. The most common types (Patterns I and II) show a background of mononuclear phagocytes with perivascular and parenchymal T-cell infiltration; Pattern II is further distinguished by immunoglobulin and complement deposition. In ~25% of biopsied active lesions (Pattern III), oligodendrocyte apoptosis is accompanied by a “dying-back” oligodendrogliopathy, starting at the “inner tongue.” These lesions show resemble viral, toxic, and ischemic processes, and can be destructive. After the acute phase, factors that remain poorly understood determine whether surviving axons in a lesion are invested by a thin myelin sheath (“remyelinated”), whether inflammation resolves without remyelination (“chronic inactive”), or whether inflammation and slow myelin degeneration persist (“smoldering”). Smoldering lesions are most common in progressive MS. The subpial cortical lesion, which is also more common in progressive MS, is characterized by demyelination of the superficial cortex, possibly associated with inflammation in the overlying leptomeninges and sparse microglia at the border between demyelinated and myelinated neuropil.
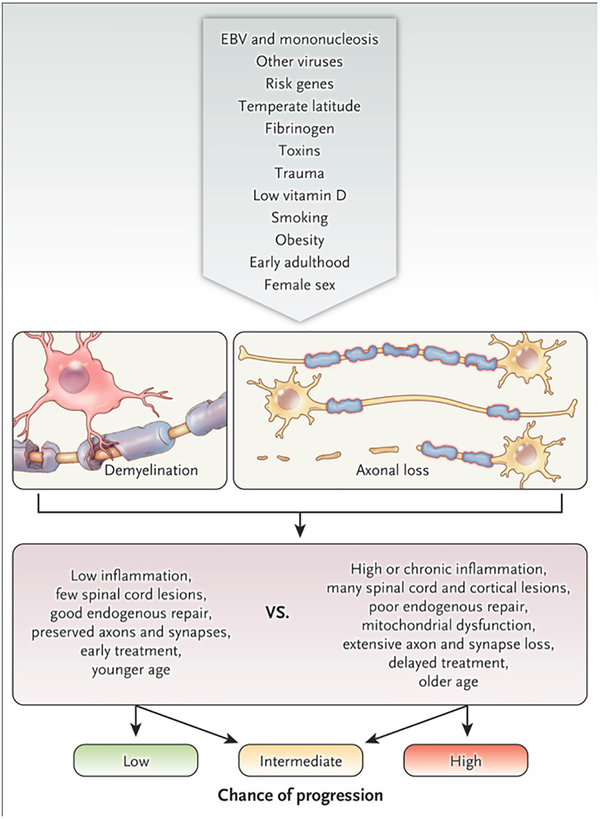
It is exceedingly unlikely that multiple sclerosis will ultimately be attributed to a single cause. Rather, the genetic and environmental factor or combination of factors that predispose to and initiate the disease, and that modify its course, are highly diverse from one person to the next. The top row of the figure depicts the funneling of proposed factors, for which varying levels of evidence exist, into the development of inflammatory, demyelinating lesions with heterogeneous axonal loss (second row). The third row lists features of the lesions and their consequences that are generally salutary or deleterious and that modify the chance of progression (bottom row).
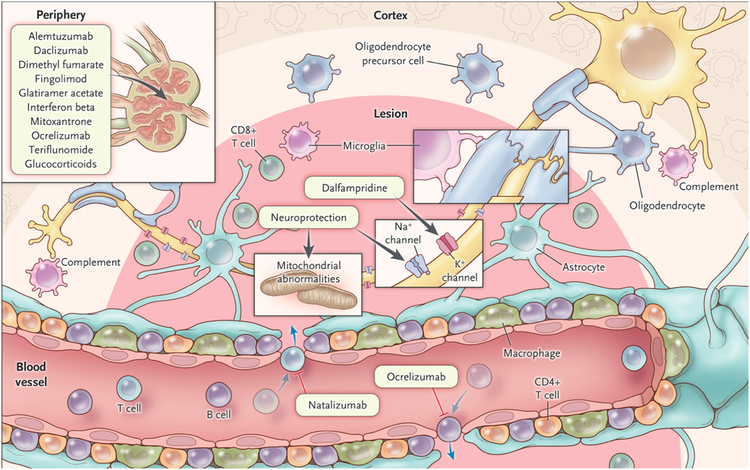
Simplified schematic depiction of major cell types within white matter MS lesions, along with several current and promising therapeutic targets in the central nervous system and in the periphery. More detailed descriptions can be found in the text.
References
-
- Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: progress and challenges. Lancet 2017;389(10076):1336–46. - PubMed
-
- Signori A, Gallo F, Bovis F, Di Tullio N, Maietta I, Sormani MP. Long-term impact of interferon or Glatiramer acetate in multiple sclerosis: A systematic review and meta-analysis. Multiple Sclerosis and Related Disorders 2016;6:57–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical