

Evaluating barriers to adopting telemedicine worldwide: A systematic review
- PMID: 29320966
- PMCID: PMC5768250
- DOI: 10.1177/1357633X16674087
Evaluating barriers to adopting telemedicine worldwide: A systematic review
Abstract
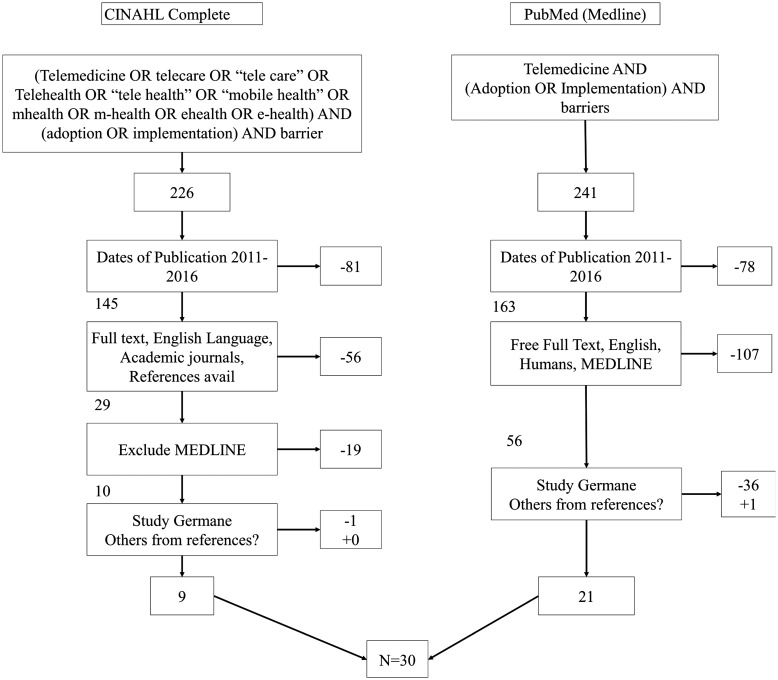
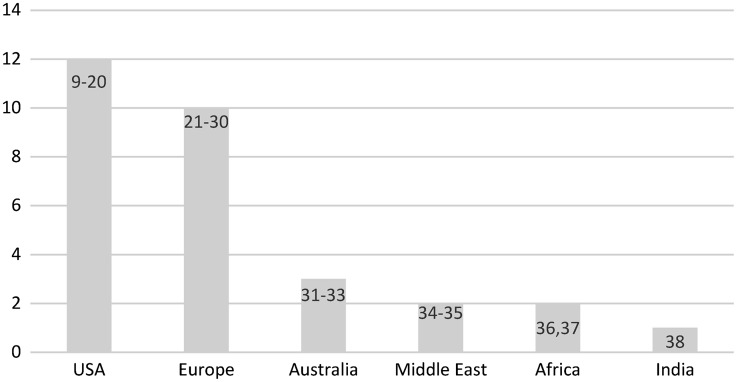
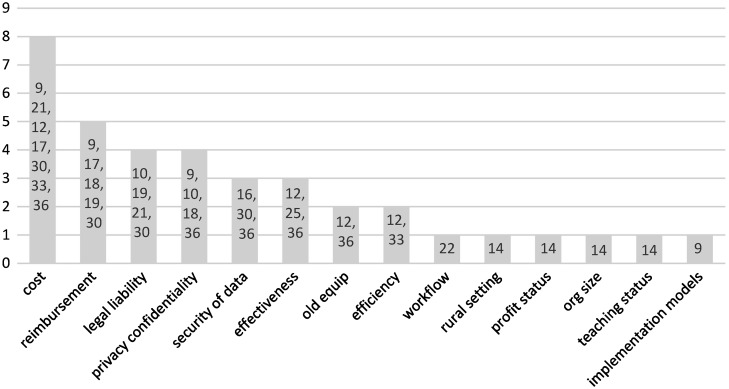
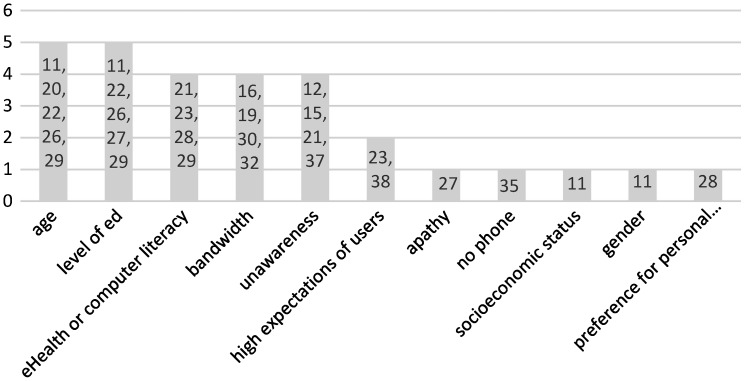
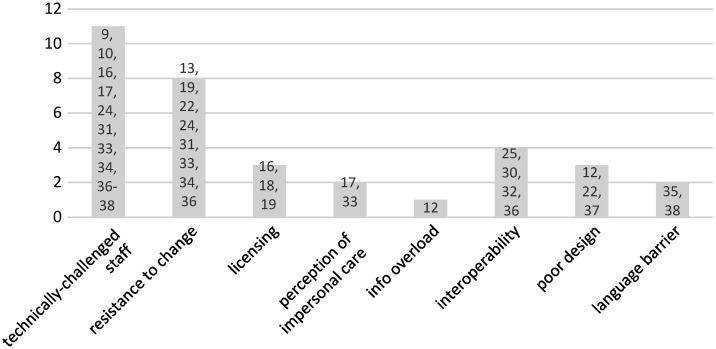
Introduction and objective Studies on telemedicine have shown success in reducing the geographical and time obstacles incurred in the receipt of care in traditional modalities with the same or greater effectiveness; however, there are several barriers that need to be addressed in order for telemedicine technology to spread. The aim of this review is to evaluate barriers to adopting telemedicine worldwide through the analysis of published work. Methods The authors conducted a systematic literature review by extracting the data from the Cumulative Index of Nursing and Allied Health Literature (CINAHL) and PubMed (MEDLINE) research databases. The reviewers in this study analysed 30 articles (nine from CINAHL and 21 from Medline) and identified barriers found in the literature. This review followed the checklist from Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009. The reviewers organized the results into one table and five figures that depict the data in different ways, organized by: barrier, country-specific barriers, organization-specific barriers, patient-specific barriers, and medical-staff and programmer-specific barriers. Results The reviewers identified 33 barriers with a frequency of 100 occurrences through the 30 articles. The study identified the issues with technically challenged staff (11%), followed by resistance to change (8%), cost (8%), reimbursement (5%), age of patient (5%), and level of education of patient (5%). All other barriers occurred at or less than 4% of the time. Discussion and conclusions Telemedicine is not yet ubiquitous, and barriers vary widely. The top barriers are technology-specific and could be overcome through training, change-management techniques, and alternating delivery by telemedicine and personal patient-to-provider interaction. The results of this study identify several barriers that could be eliminated by focused policy. Future work should evaluate policy to identify which one to lever to maximize the results.
Keywords: Barriers; adoption; implementation; mHealth; telemedicine.
Figures
References
-
- World Health Organization (WHO). Telemedicine: opportunities and developments in Member States: report on the second global survey on eHealth, Global Observatory for eHealth seires – Volume 2. NLM classification W 26.5. ISBN 9789241564144. ISSN 2220-5462. Geneva: World Health Organization, 2010.
-
- Russo JE, McCool RR, Davies L. VA telemedicine: an analysis of cost and time savings. Telemed J E Health 2016; 22(3): 209–215. - PubMed
-
- Hatcher-Martin J, Anderson E, Factor S. Patient acceptance and potential cost-savings of teleneurology in an academic outpatient movement disorders practice (P1.022). Neurology 2016; 86(Suppl 16): P1–022.
-
- Cota A, Tarchala M, Parent-Harvey C, et al. Review of 5.5 years’ experience using e-mail-based telemedicine to deliver orthopedic care to remote communities. Telemed J E Health 2017; 23(1): 37–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
