

Caesarean delivery-related blood transfusion: correlates in a tertiary hospital in Southwest Nigeria
- PMID: 29320992
- PMCID: PMC5764010
- DOI: 10.1186/s12884-017-1643-7
Caesarean delivery-related blood transfusion: correlates in a tertiary hospital in Southwest Nigeria
Abstract
Background: Caesarean delivery carries a risk of major intra-operative blood loss and its performance is often delayed by non-availability of blood and blood products. Unnecessary cross-matching and reservation of blood lead to apparent scarcity in centres with limited supply. This study set out to identify the risk factors for blood transfusion in women who underwent caesarean delivery at a tertiary obstetric unit with a view to ensuring efficient blood utilization.
Methods: A prospective cohort analysis of 906 women who had caesarean deliveries at the Lagos State University Teaching Hospital, Nigeria between January and December, 2011. A comparison was made between 188 women who underwent blood transfusion and 718 who did not. Data were obtained on a daily basis by investigators from patients, clinical notes and referral letters using structured pre-tested data collecting form. Socio-demographic characteristics; antenatal, perioperative and intraoperative details; blood loss; transfusion; and puerperal observations were recorded. EPI-Info statistical software version 3.5.3 was used for multivariable analysis to determine independent risk factors for blood transfusion.
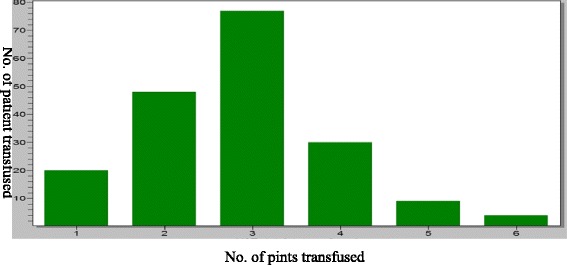
Results: Of the 2134 deliveries during the study period, 906 (42.5%) had caesarean deliveries and of which 188 (20.8%) were transfused. The modal unit of blood transfused was 3 pints (41.3%). The most common indication for caesarean section was cephalo-pelvic disproportion (25.7%).The independent risk factors for blood transfusion at caesarean section were second stage Caesarean Section (aOR = 76.14, 95% CI = 1.25-4622.06, p = 0.04), placenta previa (aOR = 32.57, 95% CI = 2.22-476.26, p = 0.01), placental abruption (aOR = 25.35, 95% CI = 3.06-211.02, p < 0.001), pre-operative anaemia (aOR = 12.15, 95% = CI 4.02-36.71, p < 0.001), prolonged operation time (aOR = 10.72 95% CI = 1.37-36.02, p < 0.001), co-morbidities like previous uterine scar (aOR = 7.02, 95% CI = 1.37-36.02, p = 0.02) and hypertensive disorders in pregnancy (aOR = 5.19, 95% CI = 1.84-14.68, p < 0.001). Obesity reduced the risk for blood transfusion (aOR = 0.24, 95% CI = 0.09-0.61, p = 0.0024).
Conclusion: The overall risk of blood transfusion in cesarean delivery is high. Paturients with the second stage Caesarean section, placenta previa, abruptio placentae and preoperative maternal anaemia have an increased risk of blood transfusion. Hence, adequate peri-operative preparations for blood transfusion are essential in these situations. Optimizing maternal hemoglobin concentration during antenatal period may reduce the incidence of caesarean-associated blood transfusion.
Keywords: Blood loss; Blood transfusion; Caesarean delivery; Case-control study; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was given by the research and ethics Committee of the Lagos State University Teaching Hospital. Consent for participation was obtained verbally from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Waterston M, Wolfe C, Hooper R, Bewley S. Postnatal morbidity after childbirth and severe obstetric morbidity. Br J ObstetGynaecol. 2003;110:728–733. - PubMed
-
- Imarengiaye CO, Ande ABA. Risk factors for blood transfusion during caesarean section in a tertiary hospital in Nigeria. Med SciMonit. 2006;12:CR269–CR272. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
