

The perceptions and experiences of women who achieved and did not achieve a waterbirth
- PMID: 29320998
- PMCID: PMC5763519
- DOI: 10.1186/s12884-017-1637-5
The perceptions and experiences of women who achieved and did not achieve a waterbirth
Abstract
Background: There is a gap in knowledge and understanding relating to the experiences of women exposed to the opportunity of waterbirth. Our aim was to explore the perceptions and experiences of women who achieved or did not achieve their planned waterbirth.
Methods: An exploratory design using critical incident techniques was conducted between December 2015 and July 2016, in the birth centre of the tertiary public maternity hospital in Western Australia. Women were telephoned 6 weeks post birth. Demographic data included: age; education; parity; and previous birth mode. Women were also asked the following: what made you choose to plan a waterbirth?; what do you think contributed to you having (or not having) a waterbirth?; and which three words would you use to describe your birth experience? Frequency distributions and univariate comparisons were employed for quantitative data. Thematic analysis was undertaken to extract common themes from the interviews.
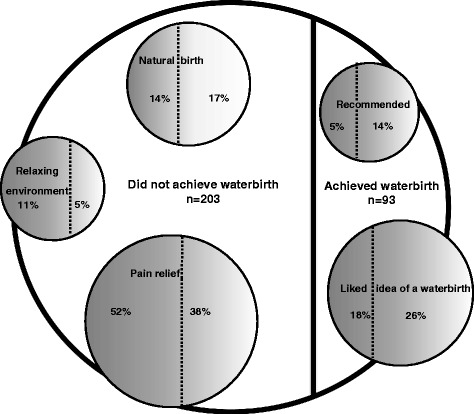
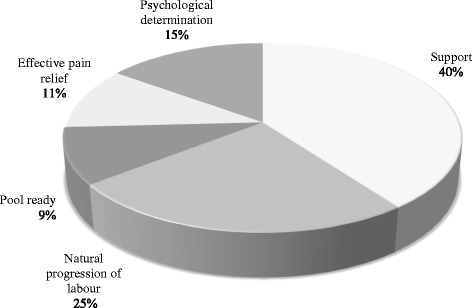
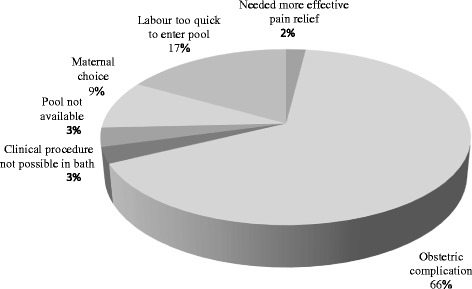
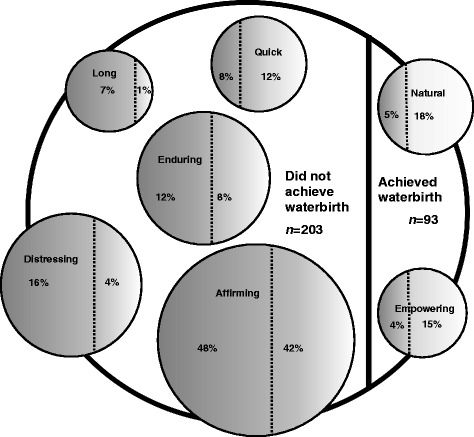
Results: A total of 31% (93 of 296) of women achieved a waterbirth and 69% (203 of 296) did not. Multiparous women were more likely to achieve a waterbirth (57% vs 32%; p < 0.001). Women who achieved a waterbirth were less likely to have planned a waterbirth for pain relief (38% vs 52%; p = 0.24). The primary reasons women gave for planning a waterbirth were: pain relief; they liked the idea; it was associated with a natural birth; it provided a relaxing environment; and it was recommended. Two fifths (40%) of women who achieved a waterbirth suggested support was the primary reason they achieved their waterbirth, with the midwife named as the primary support person by 34 of 37 women. Most (66%) women who did not achieve a waterbirth perceived this was because they experienced an obstetric complication. The words women used to describe their birth were coded as: affirming; distressing; enduring; natural; quick; empowering; and long.
Conclusions: Immersion in water for birth facilitates a shift of focus from high risk obstetric-led care to low risk midwifery-led care. It also facilitates evidence based, respectful midwifery care which in turn optimises the potential for women to view their birthing experience through a positive lens.
Keywords: Birth experience; Intrapartum care; Midwifery-led care; Waterbirth.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was gained from the Women and Newborn Ethics Committee (Approval Number 2016123QK) at the study centre. An information sheet outlining the study and informing women they may be contacted post birth was given to women at 37 weeks gestation by their midwife. Six weeks post birth women were telephoned by a research midwife not involved in their clinical care and invited to participate in the research. The study purpose was explained to all women and verbal agreement to participate in a telephone interview with the research team was considered ‘implied consent’. This method of consent was approved as women had been given an information sheet outlining the study, in addition to the study purpose being explained to all women prior to the telephone interview.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
