

Diagnostic and prognostic utility of cardiovascular magnetic resonance imaging in heart failure with preserved ejection fraction - implications for clinical trials
- PMID: 29321034
- PMCID: PMC5763769
- DOI: 10.1186/s12968-017-0424-9
Diagnostic and prognostic utility of cardiovascular magnetic resonance imaging in heart failure with preserved ejection fraction - implications for clinical trials
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) is a poorly characterized condition. We aimed to phenotype patients with HFpEF using multiparametric stress cardiovascular magnetic resonance imaging (CMR) and to assess the relationship to clinical outcomes.
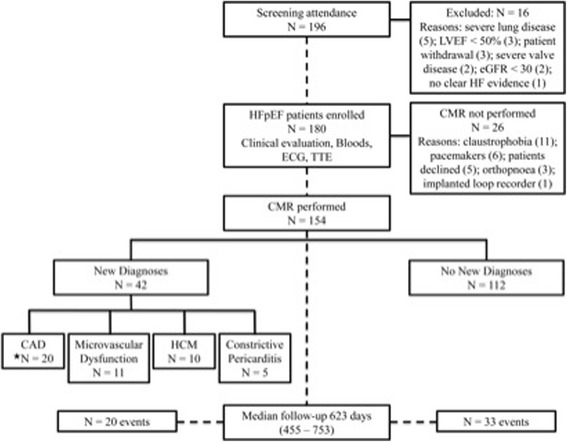
Methods: One hundred and fifty four patients (51% male, mean age 72 ± 10 years) with a diagnosis of HFpEF underwent transthoracic echocardiography and CMR during a single study visit. The CMR protocol comprised cine, stress/rest perfusion and late gadolinium enhancement imaging on a 3T scanner. Follow-up outcome data (death and heart failure hospitalization) were captured after a minimum of 6 months.
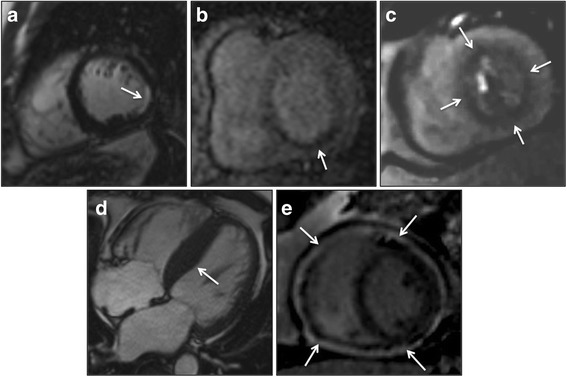
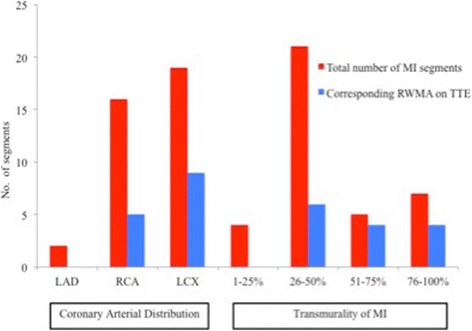
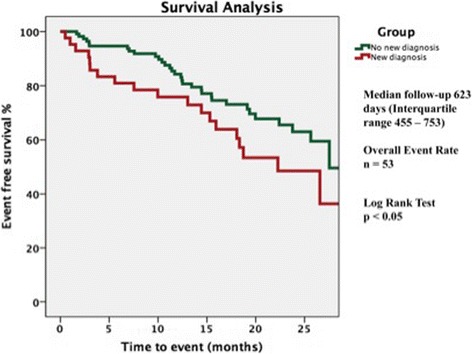
Results: CMR detected previously undiagnosed pathology in 42 patients (27%), who had similar baseline characteristics to those without a new diagnosis. These diagnoses consisted of: coronary artery disease (n = 20, including 14 with 'silent' infarction), microvascular dysfunction (n = 11), probable or definite hypertrophic cardiomyopathy (n = 10) and constrictive pericarditis (n = 5). Four patients had dual pathology. During follow-up (median 623 days), patients with a new CMR diagnosis were at higher risk of adverse outcome for the composite endpoint (log rank test: p = 0.047). In multivariate Cox proportional hazards analysis, a new CMR diagnosis was the strongest independent predictor of adverse outcome (hazard ratio: 1.92; 95% CI: 1.07 to 3.45; p = 0.03).
Conclusions: CMR diagnosed new significant pathology in 27% of patients with HFpEF. These patients were at increased risk of death and heart failure hospitalization.
Trial registration: ClinicalTrials.gov Identifier: NCT03050593 . Retrospectively registered; Date of registration: February 06, 2017.
Keywords: Cardiovascular magnetic resonance imaging; Diagnostic; Heart failure; Heart failure with preserved ejection fraction; Prognostic; Transthoracic echocardiography.
Conflict of interest statement
Ethics approval and consent to participate
All study participants provided written informed consent. The study was approved by the National Research Ethics Service Committee East Midlands – Nottingham 1 on July 24, 2012 (Reference: 12/EM/0222).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests .
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Cosyns B, Plein S, Nihoyanopoulos P, Smiseth O, Achenbach S, Andrade MJ, Pepi M, Ristic A, Imazio M, Paelinck B, et al. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur. Heart J. Cardiovasc.Imaging. 2015;16(1):12–31. doi: 10.1093/ehjci/jeu128. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
