

What is in your wallet? A cluster randomized trial of the effects of showing comparative patient out-of-pocket costs on primary care prescribing for uncomplicated hypertension
- PMID: 29321043
- PMCID: PMC5763524
- DOI: 10.1186/s13012-017-0701-x
What is in your wallet? A cluster randomized trial of the effects of showing comparative patient out-of-pocket costs on primary care prescribing for uncomplicated hypertension
Abstract
Background: Drug expenditures are responsible for an increasing proportion of health costs, accounting for $1.1 trillion in annual expenditure worldwide. As hundreds of billions of dollars are being spent each year on overtreatment with prescribed medications that are either unnecessary or are in excess of lowest cost-effective therapy, programs are needed that optimize fiscally appropriate use. We evaluated whether providing physicians with information on the patient out-of-pocket payment consequences of prescribing decisions that were in excess of lowest cost-effective therapy would alter prescribing decisions using the treatment of uncomplicated hypertension as an exemplar.
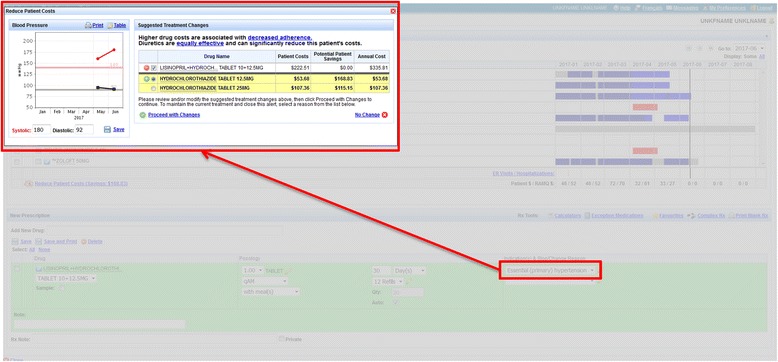
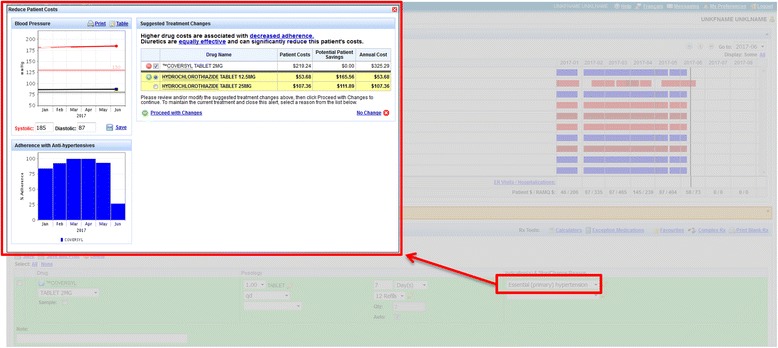
Methods: A single-blind cluster randomized trial was conducted over a 60-month follow-up period in 76 primary care physicians in Quebec, Canada, and their patients with uncomplicated hypertension who were using the MOXXI integrated electronic health record for drug and health problem management. Physicians were randomized to an out-of-pocket expenditure module that provided alerts for comparative out-of-payment costs, thiazide diuretics as recommended first-line therapy, and tools to monitor blood pressure targets and medication compliance, or alternatively the basic MOXXI system. System software and prescription claims were used to analyze the impact of the intervention on treatment choice, adherence, and overall and out-of-pocket payment costs using generalized estimating equations.
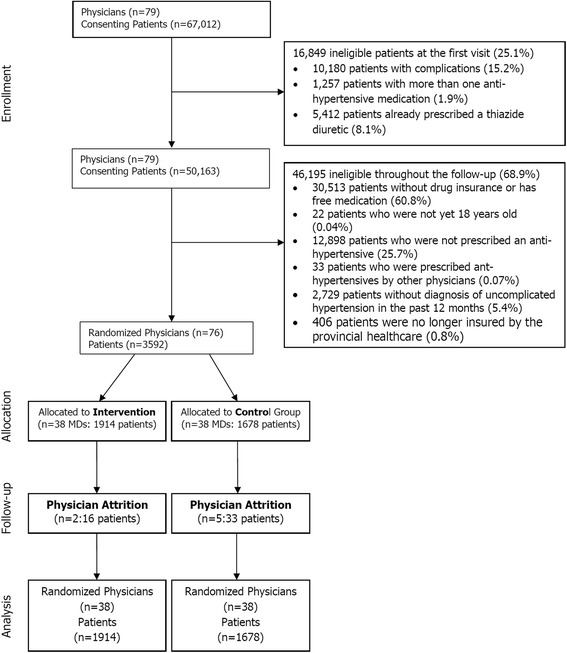
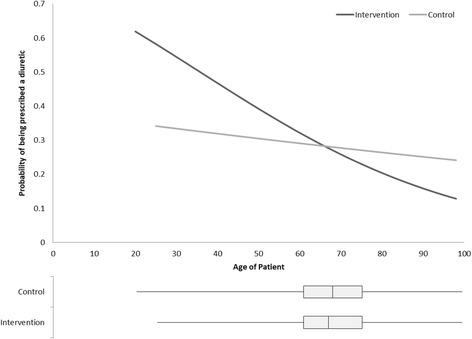
Results: Three thousand five-hundred ninety-two eligible patients with uncomplicated hypertension were enrolled, of whom 1261 (35.1%) were newly started (incident patient) on treatment during follow-up. There was a statistically significant increase in the prescription of diuretics in the newly treated intervention (26.6%) compared to control patients (19.8%) (RR 1.65, 95% CI 1.17 to 2.33). For patients already treated (prevalent patient), there was a statistically significant interaction between the intervention and patient age, with older patients being less likely to be switched to a diuretic. Among the incident patients, physicians with less than 15 years of experience were much more likely to prescribe a diuretic (OR 10.69; 95% CI 1.49 to 76.64) than physicians with 15 to 25 years (OR 0.67; 95%CI 0.25 to 1.78), or more than 25 years of experience (OR 1.80; 95% CI 1.23 to 2.65). There was no statistically significant effect of the intervention on adherence or out-of-pocket payment cost.
Conclusions: The provision of comparative information on patient out-of-pocket payments for treatment of uncomplicated hypertension had a statistically significant impact on increasing the initiation of diuretics in incident patients and switching to diuretics in younger prevalent patients. The impact of interventions to improve the cost-effectiveness of prescribing may be enhanced by also targeting patients with tools to participate in treatment decision-making and by providing physicians with comparative out-of-pocket information on all evidence-based alternatives that would enhance clinical decision-making.
Trial registration: ISRCTN96253624.
Keywords: Anti-hypertensive agents; Computerized decision support; Cost-effectiveness; Electronic prescribing.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained and maintained throughout the trial and study from the McGill Institutional Review Board (#A07-B27-06B). All patients included in the study provided consent to be included in the trial.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Information CIfH. National health expenditure trends, 1985 to 2012. Ottawa: Canadian Institute for Health Information (CFHI); 2013.
-
- PMPRB: Patented medicine prices review board annual report 2015. Edited by PMPRB. Ottawa: Patented Medicine Prices Review Board (PMPRB); 2016.
-
- Institute Q. Outlook for global medicines through 2021. Parsippany: Quintiles IMS Institute; 2016.
-
- OECD . Healthcare costs unsustainable in advanced economies without reform. 2015.
-
- Corporation AR, Mays J, Brenner M. www.kf. org. Menlo Park: The Henry J.Kaiser Family Foundation; 2004. Estimates of Medicare beneficiaries’ out-of-pocket drug spending in 2006.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
