

Insufficient sensitivity of joint aspiration during the two-stage exchange of the hip with spacers
- PMID: 29321073
- PMCID: PMC5763577
- DOI: 10.1186/s13018-017-0703-z
Insufficient sensitivity of joint aspiration during the two-stage exchange of the hip with spacers
Abstract
Background: Evaluation of infection persistence during the two-stage exchange of the hip is challenging. Joint aspiration before reconstruction is supposed to rule out infection persistence. Sensitivity and specificity of synovial fluid culture and synovial leucocyte count for detecting infection persistence during the two-stage exchange of the hip were evaluated.
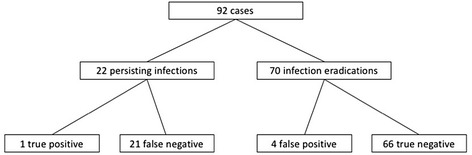
Methods: Ninety-two aspirations before planned joint reconstruction during the two-stage exchange with spacers of the hip were retrospectively analyzed.
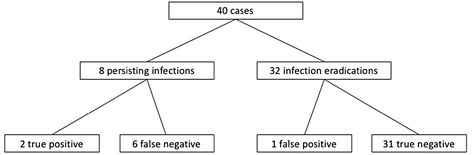
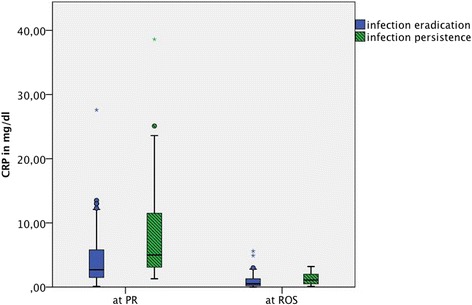
Results: The sensitivity and specificity of synovial fluid culture was 4.6 and 94.3%. The sensitivity and specificity of synovial leucocyte count at a cut-off value of 2000 cells/μl was 25.0 and 96.9%. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) values were significantly higher before prosthesis removal and reconstruction or spacer exchange (p = 0.00; p = 0.013 and p = 0.039; p = 0.002) in the infection persistence group. Receiver operating characteristic area under the curve values before prosthesis removal and reconstruction or spacer exchange for ESR were lower (0.516 and 0.635) than for CRP (0.720 and 0.671).
Conclusions: Synovial fluid culture and leucocyte count cannot rule out infection persistence during the two-stage exchange of the hip.
Keywords: Hip; Joint aspiration; Periprosthetic infection; Spacer; Two-stage exchange.
Conflict of interest statement
Authors’ information
Not applicable
Ethics approval and consent to participate
Ethics approval was confirmed by the Ethics Commission of the Medical Faculty of the University of Wuerzburg, Germany (Reference number 2016072801). Patient’s consent to participate was not required in this retrospective study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Anual Report 2017 National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. 2017. http://www.njrreports.org.uk 14th Annual Report 2017.pdf. Accessed 2017/10/07.
-
- Kapadia BH, Berg RA, Daley JA, Fritz J, Bhave A, Mont MA. Periprosthetic joint infection. Lancet. 2015;23(10016):386–394. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
