

Differentiating Primary, Genetic, and Secondary FSGS in Adults: A Clinicopathologic Approach
- PMID: 29321142
- PMCID: PMC5827609
- DOI: 10.1681/ASN.2017090958
Differentiating Primary, Genetic, and Secondary FSGS in Adults: A Clinicopathologic Approach
Abstract
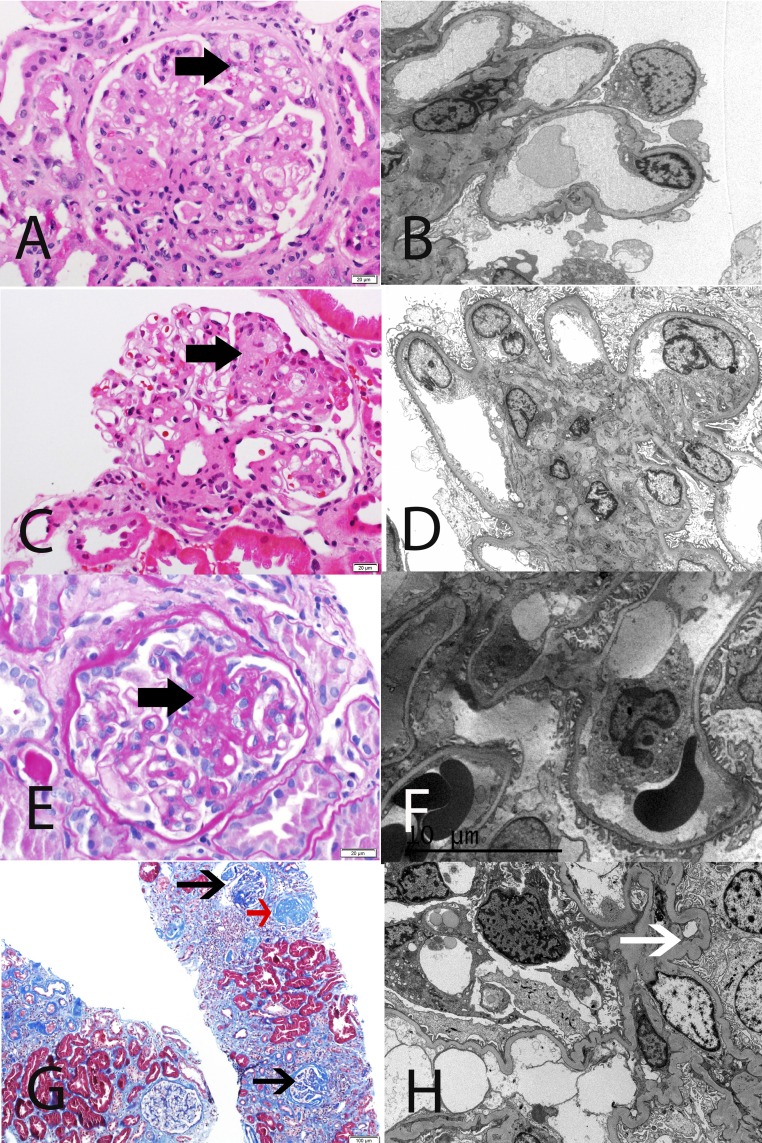
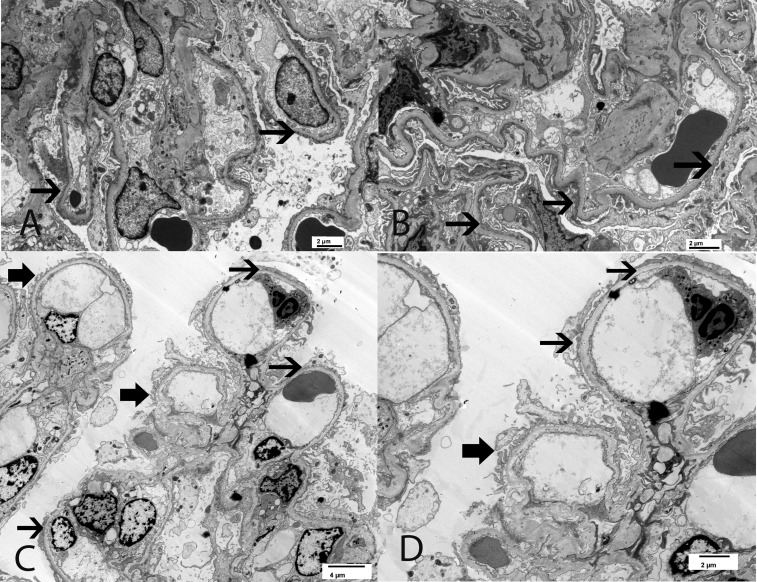
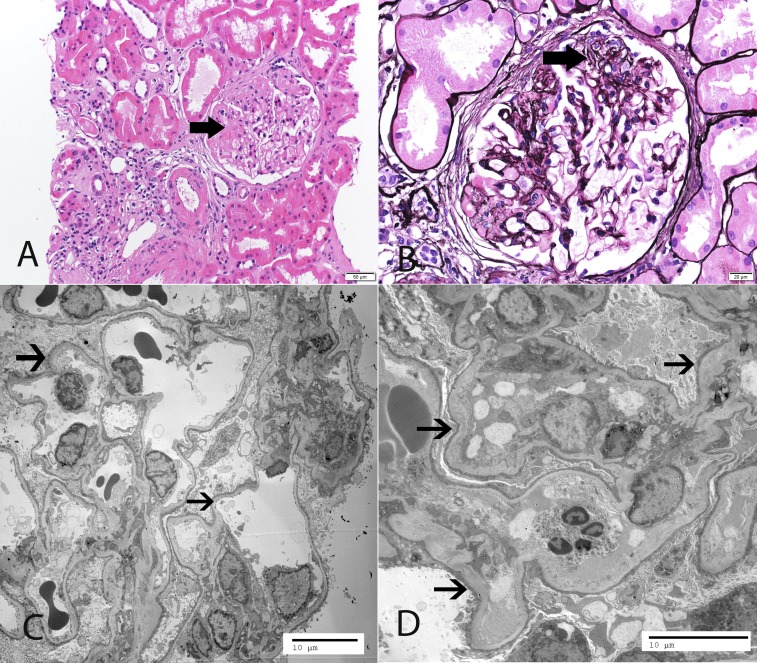
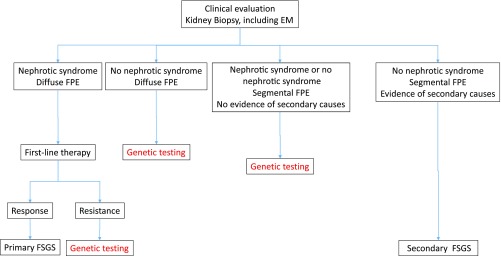
FSGS describes a renal histologic lesion with diverse causes and pathogenicities that are linked by podocyte injury and depletion. Subclasses of FSGS include primary, genetic, and secondary forms, the latter comprising maladaptive, viral, and drug-induced FSGS. Despite sharing certain clinical and histologic features, these subclasses differ noticeably in management and prognosis. Without an accepted nongenetic biomarker that discriminates among these FSGS types, classification of patients is often challenging. This review summarizes the clinical and histologic features, including the onset and severity of proteinuria as well as the presence of nephrotic syndrome, that may aid in identifying the specific FSGS subtype. The FSGS lesion is characterized by segmental sclerosis and must be differentiated from nonspecific focal global glomerulosclerosis. No light microscopic features are pathognomonic for a particular FSGS subcategory. The characteristics of podocyte foot process effacement on electron microscopy, while helpful in discriminating between primary and maladaptive FSGS, may be of little utility in detecting genetic forms of FSGS. When FSGS cannot be classified by clinicopathologic assessment, genetic analysis should be offered. Next generation DNA sequencing enables cost-effective screening of multiple genes simultaneously, but determining the pathogenicity of a detected genetic variant may be challenging. A more systematic evaluation of patients, as suggested herein, will likely improve therapeutic outcomes and the design of future trials in FSGS.
Keywords: FSGS; Primary; Secondary; genetic renal disease; nephrotic syndrome.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- D’Agati VD, Fogo AB, Bruijn JA, Jennette JC: Pathologic classification of focal segmental glomerulosclerosis: A working proposal. Am J Kidney Dis 43: 368–382, 2004 - PubMed
-
- Kachurina N, Chung CF, Benderoff E, Babayeva S, Bitzan M, Goodyer P, Kitzler T, Matar D, Cybulsky AV, Alachkar N, Torban E: Novel unbiased assay for circulating podocyte-toxic factors associated with recurrent focal segmental glomerulosclerosis. Am J Physiol Renal Physiol 310: F1148–F1156, 2016 - PubMed
-
- Allard L, Kwon T, Krid S, Bacchetta J, Garnier A, Novo R, Deschenes G, Salomon R, Roussey G, Allain-Launay E: Treatment by immunoadsorption for recurrent focal segmental glomerulosclerosis after paediatric kidney transplantation: A multicentre French cohort [published online ahead of print July 28, 2017]. Nephrol Dial Transplant 10.1093/ndt/gfx214 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
