

Differences in risk factors for 3 types of stroke: UK prospective study and meta-analyses
- PMID: 29321237
- PMCID: PMC5798656
- DOI: 10.1212/WNL.0000000000004856
Differences in risk factors for 3 types of stroke: UK prospective study and meta-analyses
Abstract
Objective: To compare associations of behavioral and related factors for incident subarachnoid hemorrhage and intracerebral hemorrhage and ischemic stroke.
Methods: A total of 712,433 Million Women Study participants without prior stroke, heart disease, or cancer reported behavioral and related factors at baseline (1999-2007) and were followed up by record linkage to national hospital admission and death databases. Cox regression yielded adjusted relative risks (RRs) by type of stroke. Heterogeneity was assessed with χ2 tests. When appropriate, meta-analyses were done of published prospective studies.
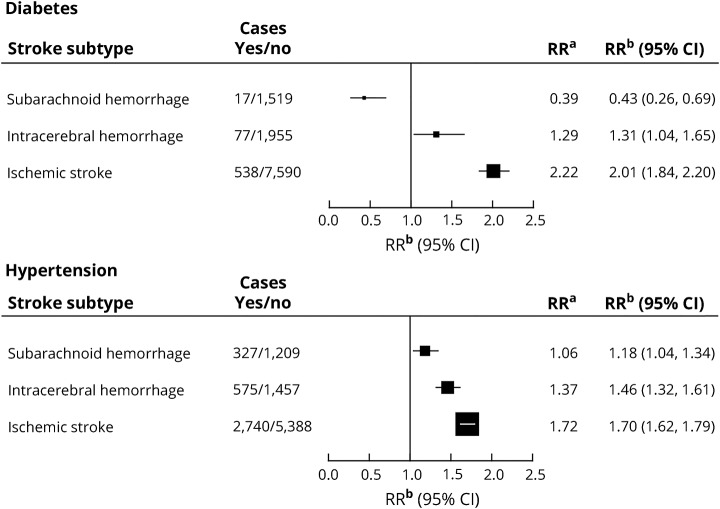
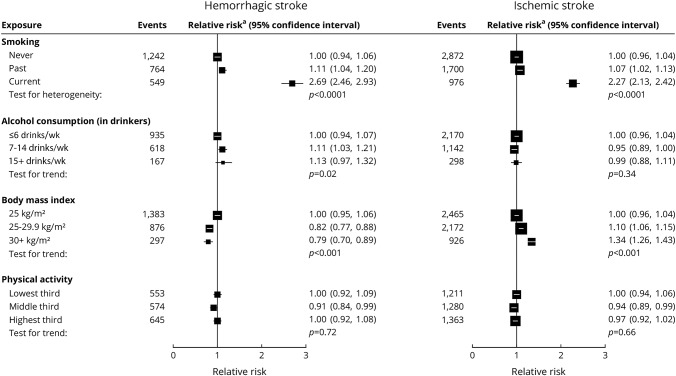
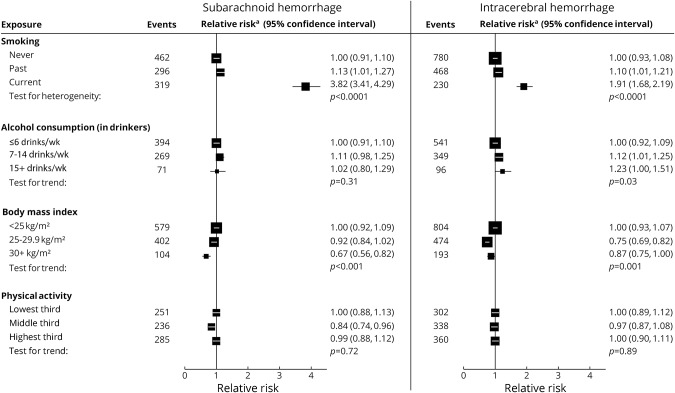
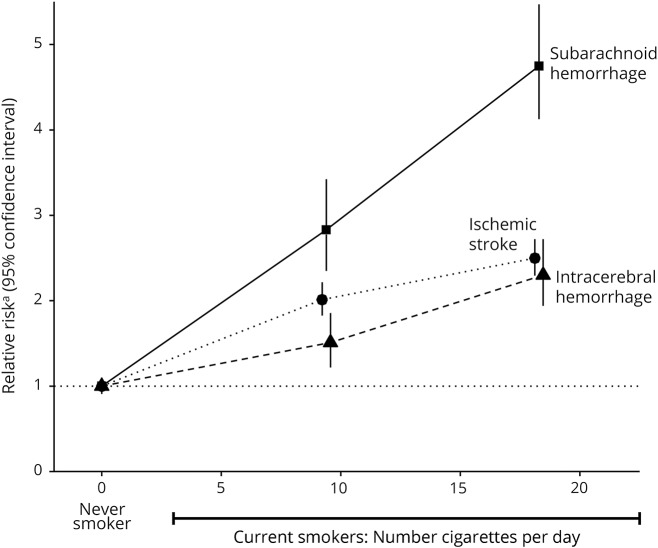
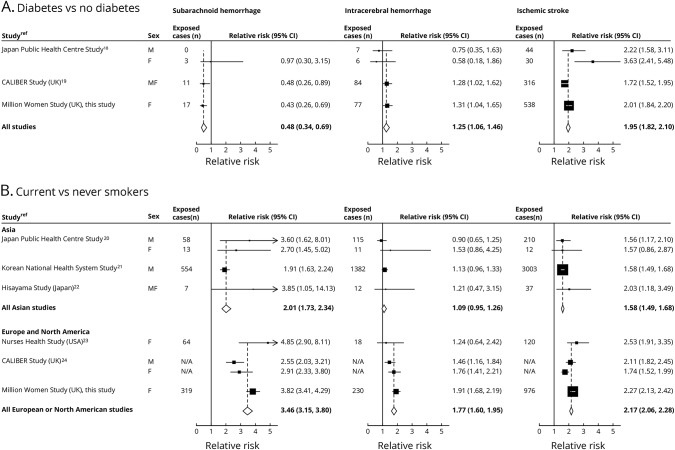
Results: After 12.9 (SD 2.6) years of follow-up, 8,128 women had an incident ischemic stroke, 2,032 had intracerebral hemorrhage, and 1,536 had subarachnoid hemorrhage. In women with diabetes mellitus, the risk of ischemic stroke was substantially increased (RR 2.01, 95% confidence interval [CI] 1.84-2.20), risk of intracerebral hemorrhage was increased slightly (RR 1.31, 95% CI 1.04-1.65), but risk of subarachnoid hemorrhage was reduced (RR 0.43, 95% CI 0.26-0.69) (heterogeneity by stroke type, p < 0.0001). Stroke incidence was greater in women who rated their health as poor/fair compared to those who rated their health as excellent/good (RR 1.36, 95% CI 1.30-1.42). Among 565,850 women who rated their heath as excellent/good, current smokers were at an increased risk of all 3 stroke types, (although greater for subarachnoid hemorrhage [≥15 cigarettes/d vs never smoker, RR 4.75, 95% CI 4.12-5.47] than for intracerebral hemorrhage [RR 2.30, 95% CI 1.94-2.72] or ischemic stroke [RR 2.50, 95% CI 2.29-2.72]; heterogeneity p < 0.0001). Obesity was associated with an increased risk of ischemic stroke and a decreased risk of hemorrhagic stroke (heterogeneity p < 0.0001). Meta-analyses confirmed the associations and the heterogeneity across the 3 types of stroke.
Conclusion: Classic risk factors for stroke have considerably different effects on the 3 main pathologic types of stroke.
Copyright © 2018 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Bennett DA, Krishnamurthi RV, Barker-Collo S, et al. . The global burden of ischemic stroke: findings of the GBD 2010 study. Glob Heart 2014;9:107–112. - PubMed
-
- Krishnamurthi RV, Moran AE, Forouzanfar MH, et al. . The global burden of hemorrhagic stroke: a summary of findings from the GBD 2010 study. Glob Heart 2014;9:101–106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical