

Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients With Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial
- PMID: 29322167
- PMCID: PMC5838601
- DOI: 10.1001/jamacardio.2017.4973
Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients With Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial
Abstract
Importance: Coronary computed tomographic angiography (coronary CTA) can characterize coronary artery disease, including high-risk plaque. A noninvasive method of identifying high-risk plaque before major adverse cardiovascular events (MACE) could provide practice-changing optimizations in coronary artery disease care.
Objective: To determine whether high-risk plaque detected by coronary CTA was associated with incident MACE independently of significant stenosis (SS) and cardiovascular risk factors.
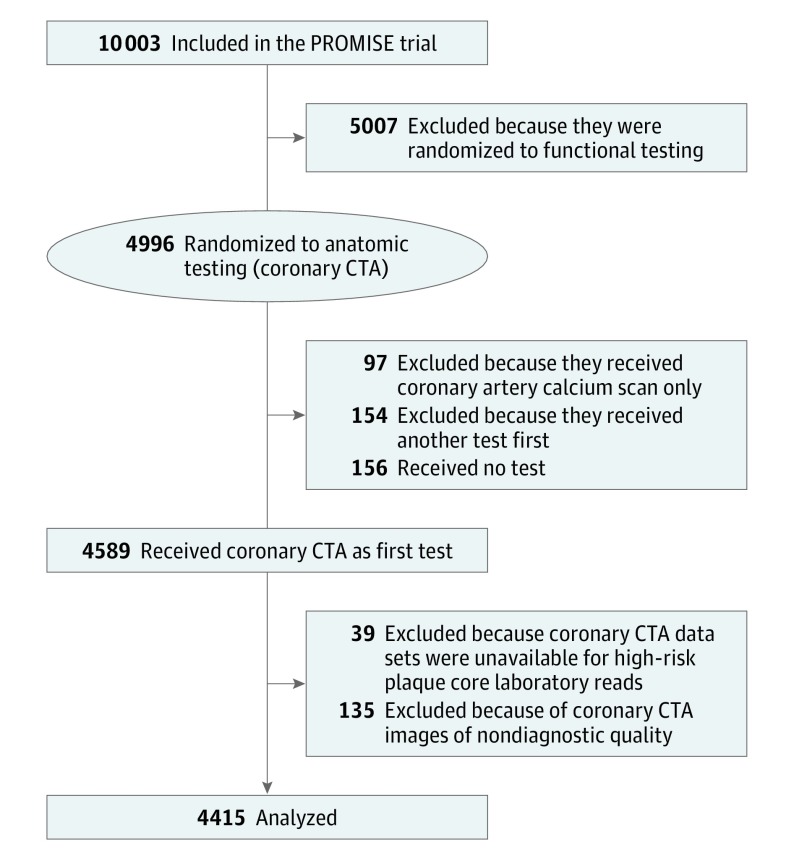
Design, setting, and participants: This prespecified nested observational cohort study was part of the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) trial. All stable, symptomatic outpatients in this trial who required noninvasive cardiovascular testing and received coronary CTA were included and followed up for a median of 25 months.
Exposures: Core laboratory assessment of coronary CTA for SS and high-risk plaque (eg, positive remodeling, low computed tomographic attenuation, or napkin-ring sign).
Main outcomes and measures: The primary end point was an adjudicated composite of MACE (defined as death, myocardial infarction, or unstable angina).
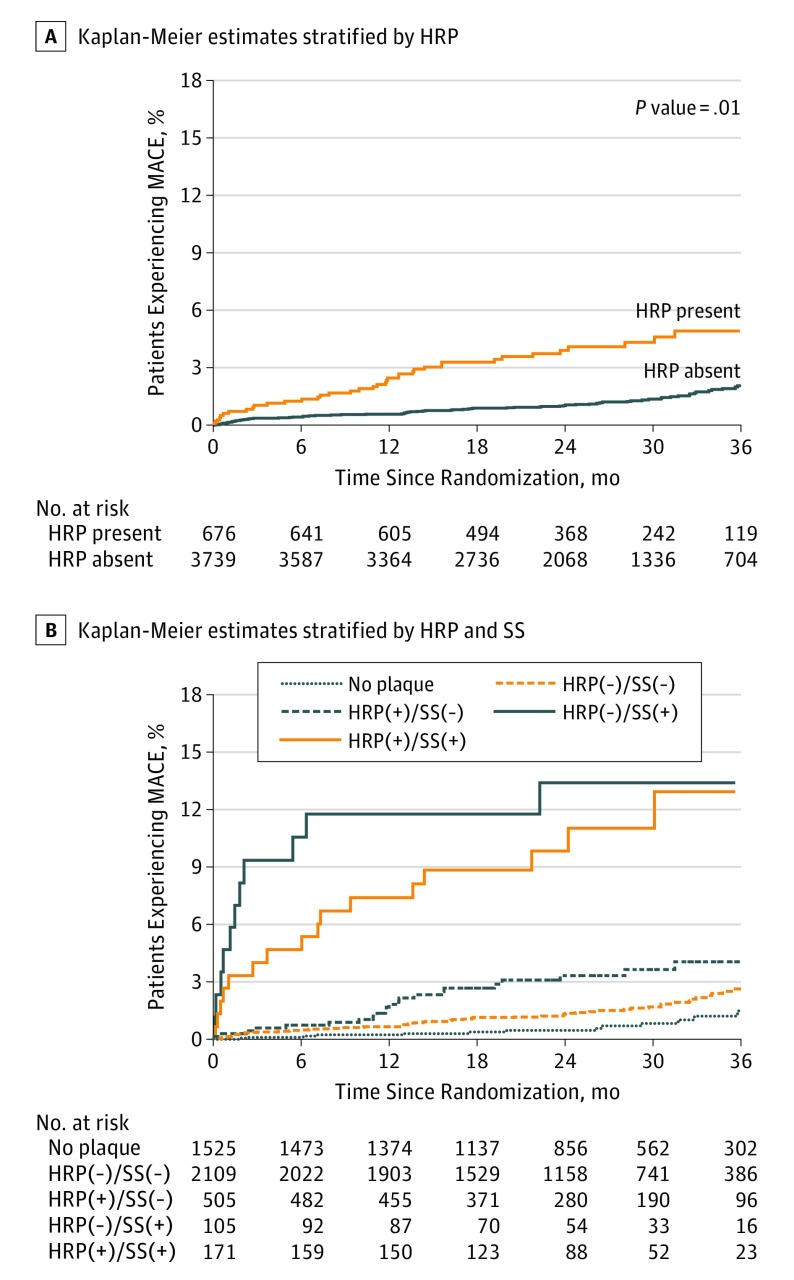
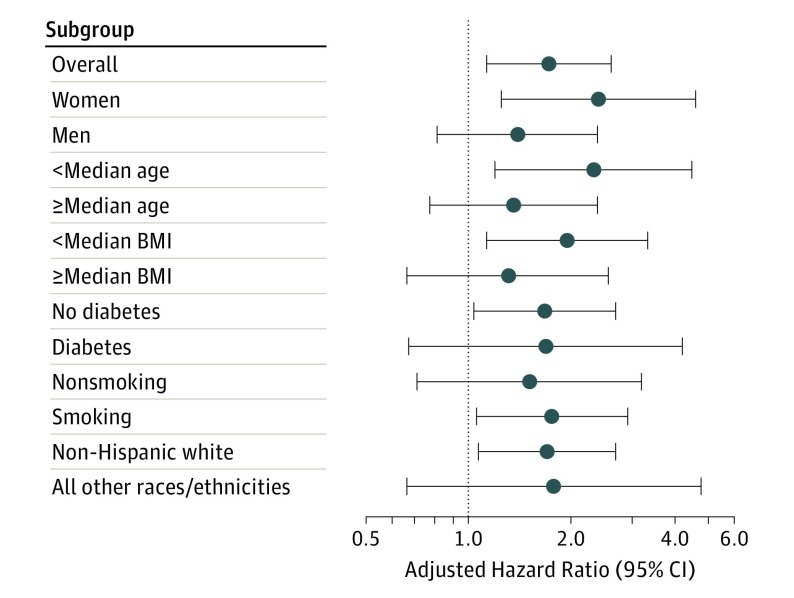
Results: The study included 4415 patients, of whom 2296 (52%) were women, with a mean age of 60.5 years, a median atherosclerotic cardiovascular disease (ASCVD) risk score of 11, and a MACE rate of 3% (131 events). A total of 676 patients (15.3%) had high-risk plaques, and 276 (6.3%) had SS. The presence of high-risk plaque was associated with a higher MACE rate (6.4% vs 2.4%; hazard ratio, 2.73; 95% CI, 1.89-3.93). This association persisted after adjustment for ASCVD risk score and SS (adjusted hazard ratio [aHR], 1.72; 95% CI, 1.13-2.62). Adding high-risk plaque to the ASCVD risk score and SS assessment led to a significant continuous net reclassification improvement (0.34; 95% CI, 0.02-0.51). Presence of high-risk plaque increased MACE risk among patients with nonobstructive coronary artery disease relative to patients without high-risk plaque (aHR, 4.31 vs 2.64; 95% CI, 2.25-8.26 vs 1.49-4.69). There were no significant differences in MACE in patients with SS and high-risk plaque as opposed to those with SS but not high-risk plaque (aHR, 8.68 vs. 9.31; 95% CI, 4.25-17.73 vs 4.21-20.61). High-risk plaque was a stronger predictor of MACE in women (aHR, 2.41; 95% CI, 1.25-4.64) vs men (aHR, 1.40; 95% CI, 0.81-2.39) and younger patients (aHR, 2.33; 95% CI, 1.20-4.51) vs older ones (aHR, 1.36; 95% CI, 0.77-2.39).
Conclusions and relevance: High-risk plaque found by coronary CTA was associated with a future MACE in a large US population of outpatients with stable chest pain. High-risk plaque may be an additional risk stratification tool, especially in patients with nonobstructive coronary artery disease, younger patients, and women. The importance of findings is limited by low absolute MACE rates and low positive predictive value of high-risk plaque.
Trial registration: clinicaltrials.gov Indentifier: NCT01174550.
Conflict of interest statement
Figures
Comment in
-
High-Risk Coronary Atherosclerotic Plaque Assessment by Coronary Computed Tomography Angiography-Should We Use It?JAMA Cardiol. 2018 Feb 1;3(2):153-154. doi: 10.1001/jamacardio.2017.5016. JAMA Cardiol. 2018. PMID: 29322177 No abstract available.
-
High-risk atherosclerotic plaque features for cardiovascular risk assessment in the Prospective Multicenter Imaging Study for Evaluation of Chest Pain trial.Cardiovasc Diagn Ther. 2019 Feb;9(1):89-93. doi: 10.21037/cdt.2018.08.09. Cardiovasc Diagn Ther. 2019. PMID: 30881885 Free PMC article. No abstract available.
References
-
- Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008;52(21):1724-1732. - PubMed
-
- Meijboom WB, Meijs MFL, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52(25):2135-2144. - PubMed
-
- Miller JM, Rochitte CE, Dewey M, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359(22):2324-2336. - PubMed
-
- SCOT-HEART investigators CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385(9985):2383-2391. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
