

S(+)-ketamine : Current trends in emergency and intensive care medicine
- PMID: 29322377
- PMCID: PMC6061669
- DOI: 10.1007/s00508-017-1299-3
S(+)-ketamine : Current trends in emergency and intensive care medicine
Erratum in
-
Correction to: S(+)-ketamine : Current trends in emergency and intensive caremedicine.Wien Klin Wochenschr. 2018 Sep;130(17-18):557. doi: 10.1007/s00508-018-1354-8. Wien Klin Wochenschr. 2018. PMID: 29959526 Free PMC article.
Abstract
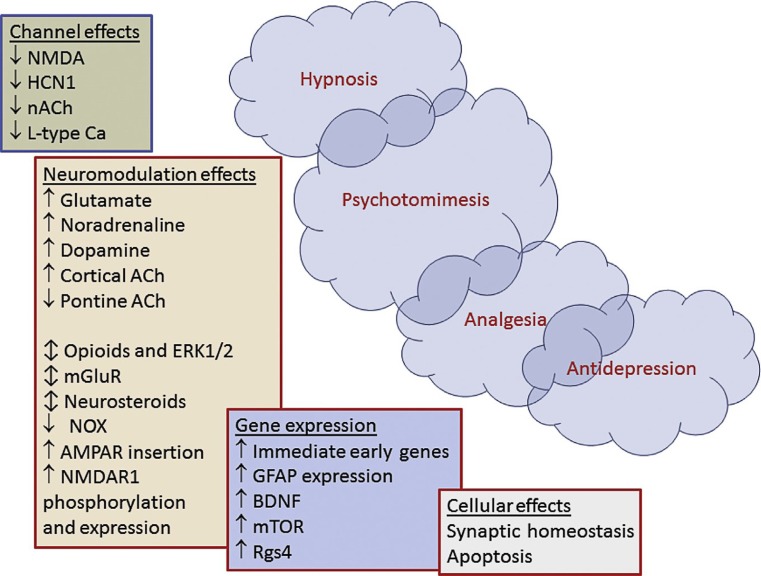
S(+)-ketamine, the pure dextrorotatory enantiomer of ketamine has been available for clinical use in analgesia and anesthesia for more than 25 years. The main effects are mediated by non-competitive inhibition of the N-methyl-D-aspartate (NMDA) receptor but S(+)-ketamine also interacts with opioid receptors, monoamine receptors, adenosine receptors and other purinergic receptors. Effects on α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors, metabotropic glutamate receptors (mGluR) and L‑type calcium chanels have also been described. S(+)-ketamine stimulates the sympathetic nerve system, making it an ideal drug for analgosedation or induction of anesthesia in instable patients. In addition, the neuroprotective properties, bronchodilatory, antihyperalgesic or antiepileptic effects provide interesting therapeutic options. In this article we discuss the numerous effects of S(+)-ketamine under pharmacological and clinical aspects especially for typical indications in emergency medicine as well as intensive care.
Keywords: Analgesia; Critical care; Emergency medicine; Ketamine; Neuroprotection.
Conflict of interest statement
H. Trimmel, R. Helbok, T. Staudinger, W. Jaksch, B. Messerer, H. Schöchl and R. Likar declare that they have no competing interests.
Figures
References
-
- Sleigh J, Harvey M, Voss L, Denny B. Ketamine—More mechanisms of action than just NMDA blockade. Trends Anaesth Crit Care. 2014;4:76–81. doi: 10.1016/j.tacc.2014.03.002. - DOI
-
- Kolawole IK. Ketamine hydrochloride: a useful but frequently misused drug. Niger J Surg Res. 2001;3:118–125.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
