

Updating osteoimmunology: regulation of bone cells by innate and adaptive immunity
- PMID: 29323344
- PMCID: PMC5821527
- DOI: 10.1038/nrrheum.2017.213
Updating osteoimmunology: regulation of bone cells by innate and adaptive immunity
Abstract
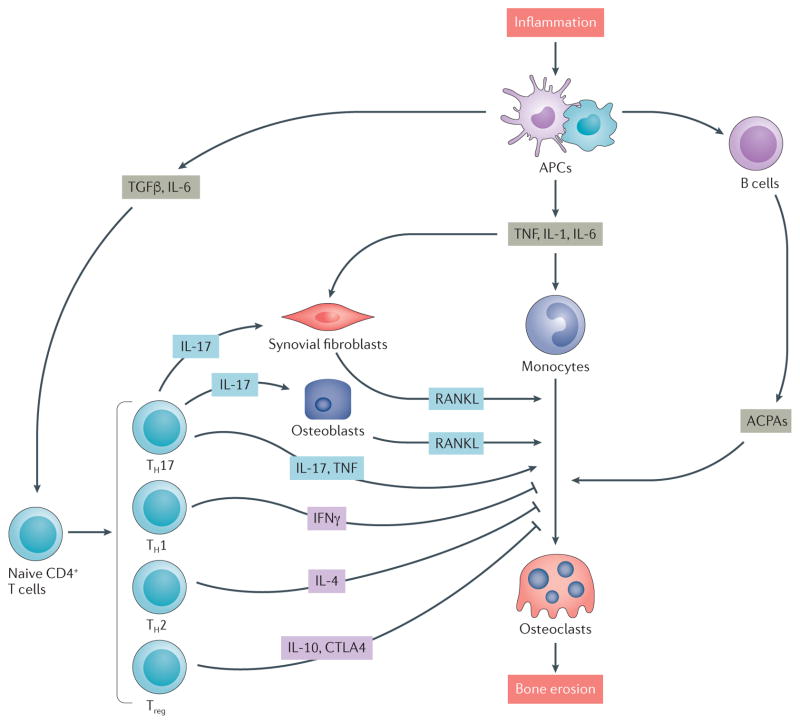
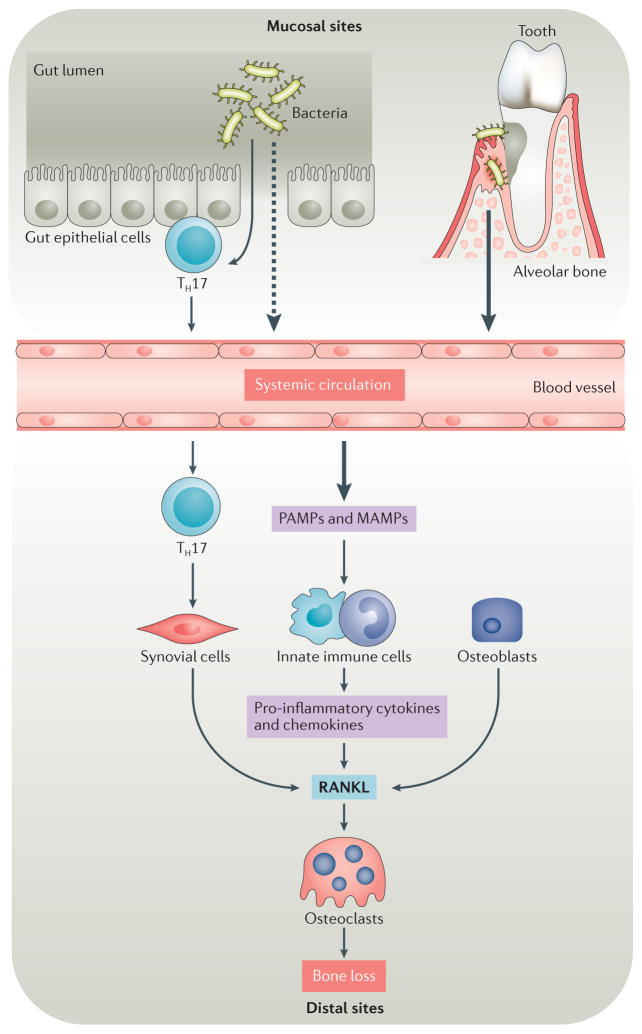
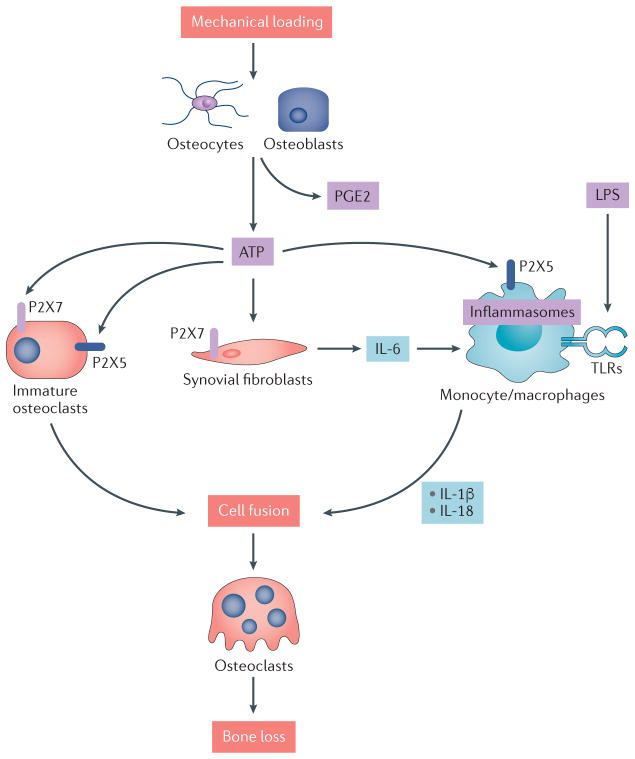
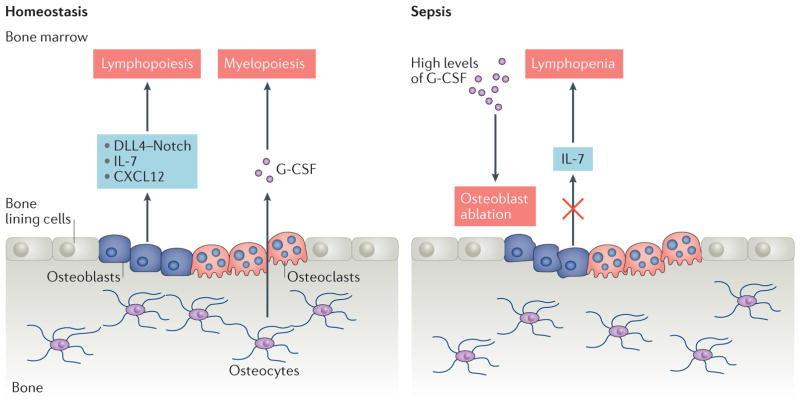
Osteoimmunology encompasses all aspects of the cross-regulation of bone and the immune system, including various cell types, signalling pathways, cytokines and chemokines, under both homeostatic and pathogenic conditions. A number of key areas are of increasing interest and relevance to osteoimmunology researchers. Although rheumatoid arthritis has long been recognized as one of the most common autoimmune diseases to affect bone integrity, researchers have focused increased attention on understanding how molecular triggers and innate signalling pathways (such as Toll-like receptors and purinergic signalling pathways) related to pathogenic and/or commensal microbiota are relevant to bone biology and rheumatic diseases. Additionally, although most discussions relating to osteoimmune regulation of homeostasis and disease have focused on the effects of adaptive immune responses on bone, evidence exists of the regulation of immune cells by bone cells, a concept that is consistent with the established role of the bone marrow in the development and homeostasis of the immune system. The active regulation of immune cells by bone cells is an interesting emerging component of investigations that seek to understand how to control immune-associated diseases of the bone and joints.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Arron JR, Choi Y. Bone versus immune system. Nature. 2000;408:535–536. - PubMed
-
- Walsh MC, et al. Osteoimmunology: interplay between the immune system and bone metabolism. Annu Rev Immunol. 2006;24:33–63. - PubMed
-
- Ash P, Loutit JF, Townsend KM. Osteoclasts derived from haematopoietic stem cells. Nature. 1980;283:669–670. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
