

Parafibromin-deficient (HPT-JT Type, CDC73 Mutated) Parathyroid Tumors Demonstrate Distinctive Morphologic Features
- PMID: 29324469
- PMCID: PMC6296846
- DOI: 10.1097/PAS.0000000000001017
Parafibromin-deficient (HPT-JT Type, CDC73 Mutated) Parathyroid Tumors Demonstrate Distinctive Morphologic Features
Abstract
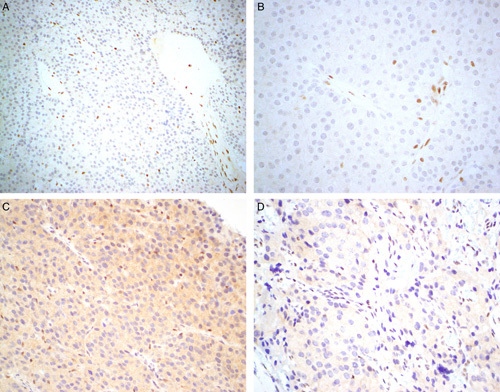
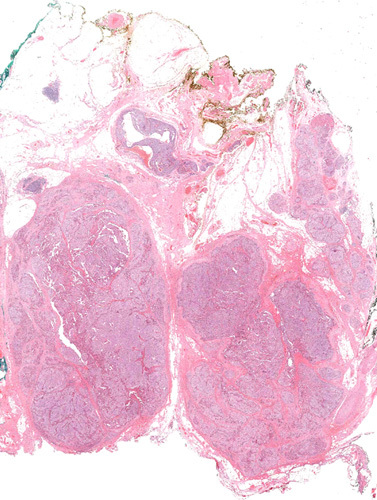
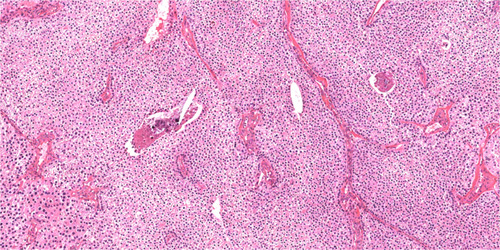
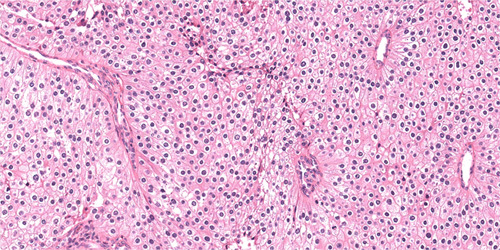
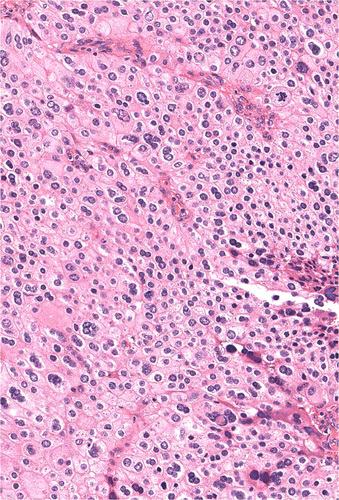
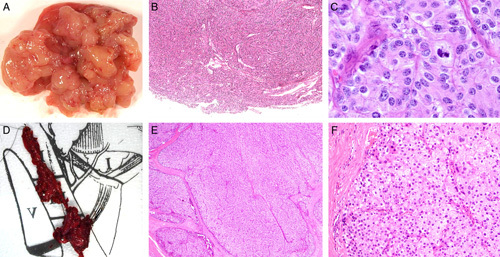
The gene CDC73 (previously known as HRPT2) encodes the protein parafibromin. Biallelic mutation of CDC73 is strongly associated with malignancy in parathyroid tumors. Heterozygous germline mutations cause hyperparathyroidism jaw tumor syndrome,which is associated with a high life-time risk of parathyroid carcinoma. Therefore loss of parafibromin expression by immunohistochemistry may triage genetic testing for hyperparathyroidism jaw tumor syndrome and be associated with malignant behavior in atypical parathyroid tumors. We share our experience that parafibromin-negative parathyroid tumors show distinctive morphology. We searched our institutional database for parathyroid tumors demonstrating complete loss of nuclear expression of parafibromin with internal positive controls. Forty-three parafibromin-negative tumors from 40 (5.1%) of 789 patients undergoing immunohistochemistry were identified. Thirty-three (77%) were external consultation cases; the estimated incidence in unselected tumors was 0.19%. Sixteen (37.2%) fulfilled World Health Organization 2017 criteria for parathyroid carcinoma and 63% had serum calcium greater than 3mmol/L. One of 27 (3.7%) noninvasive but parafibromin-negative tumors subsequently metastasized. Parafibromin-negative patients were younger (mean, 36 vs. 63 y; P<0.001) and had larger tumors (mean, 3.04 vs. 0.62 g; P<0.001). Not all patients had full testing, but 26 patients had pathogenic CDC73 mutation/deletions confirmed in tumor (n=23) and/or germline (n=16). Parafibromin-negative tumors demonstrated distinctive morphology including extensive sheet-like rather than acinar growth, eosinophilic cytoplasm, nuclear enlargement with distinctive coarse chromatin, perinuclear cytoplasmic clearing, a prominent arborizing vasculature, and, frequently, a thick capsule. Microcystic change was found in 21 (48.8%). In conclusion, there are previously unrecognized morphologic clues to parafibromin loss/CDC73 mutation in parathyroid tumors which, given the association with malignancy and syndromic disease, are important to recognize.
Conflict of interest statement
Conflicts of Interest and Source of Funding: The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Figures
References
-
- Gill AJ, Clarkson A, Gimm O, et al. Loss of nuclear expression of parafibromin distinguishes parathyroid carcinomas and hyperparathyroidsim-jaw tumor (HPT-JT) syndrome related adenomas from sporadic parathyroid adenomas and hyperplasias. Am J Surg Pathol. 2006;30:1140–1149. - PubMed
-
- Gill AJ. Understanding the genetic basis of parathyroid carcinoma. Endocr Pathol. 2014;25:30–34. - PubMed
-
- Hahn MA, Marsh DJ. Identification of a functional bipartite localization signal in the tumor suppressor parafibromin. Oncogene. 2005;15:6241–6248. - PubMed
-
- Jo JH, Chung TM, Youn H, et al. Cytoplasmic parafibromin/hCdc73 targets and destabilizes p53 mRNA to control p53-mediated apoptosis. Nat Commun. 2014;12:5433. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
