

Complications Associated With Mortality in the National Surgical Quality Improvement Program Database
- PMID: 29324497
- PMCID: PMC6150605
- DOI: 10.1213/ANE.0000000000002799
Complications Associated With Mortality in the National Surgical Quality Improvement Program Database
Abstract
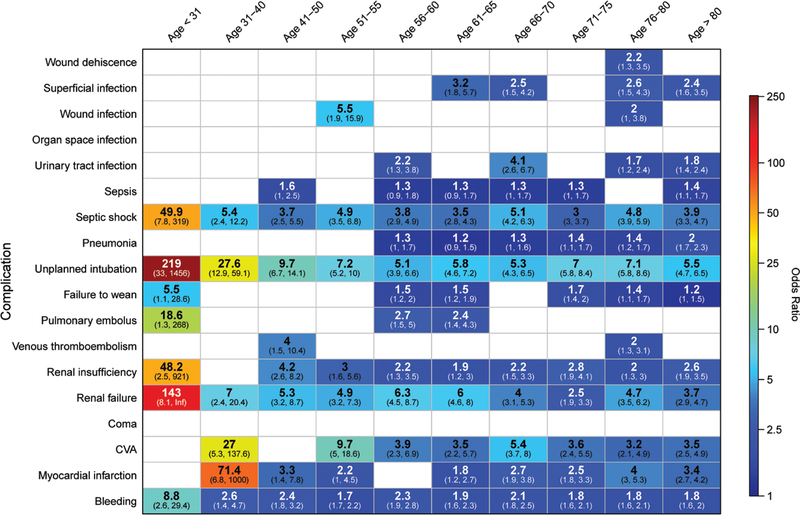
Background: Attributing causes of postoperative mortality is challenging, as death may be multifactorial. A better understanding of complications that occur in patients who die is important, as it allows clinicians to focus on the most impactful complications. We sought to determine the postoperative complications with the strongest independent association with 30-day mortality.
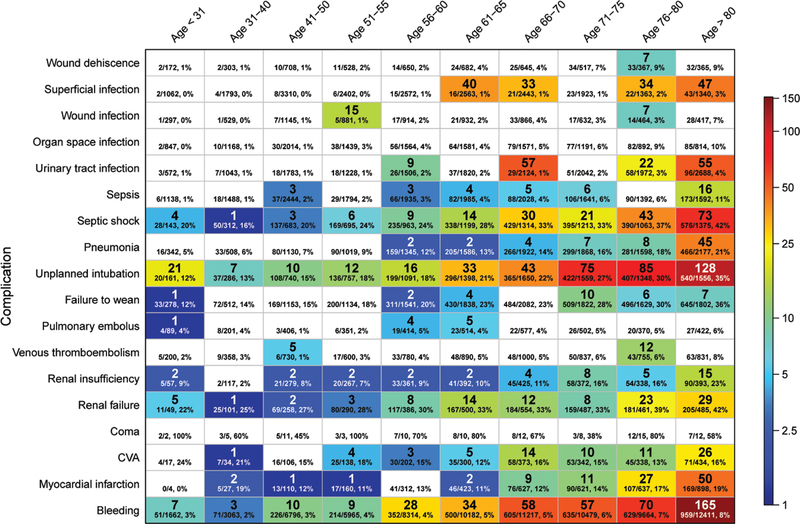
Methods: Data were obtained from the 2012-2013 National Surgical Quality Improvement Program Participant Use Data Files. All inpatient or admit day of surgery cases were eligible for inclusion in this study. A multivariable least absolute shrinkage and selection operator regression analysis was used to adjust for patient pre- and intraoperative risk factors for mortality. Attributable mortality was calculated using the population attributable fraction method: the ratio between the odds ratio for mortality and a given complication in the population. Patients were separated into 10 age groups to facilitate analysis of age-related differences in mortality.
Results: A total of 1,195,825 patients were analyzed, and 9255 deceased within 30 days (0.77%). A complication independently associated with attributable mortality was found in 1887 cases (20%). The most common causes of attributable mortality (attributable deaths per million patients) were bleeding (n = 368), respiratory failure (n = 358), septic shock (n = 170), and renal failure (n = 88). Some complications, such as urinary tract infection and pneumonia, were associated with attributable mortality only in older patients.
Discussion: Additional resources should be focused on complications associated with the largest attributable mortality, such as respiratory failure and infections. This is particularly important for complications disproportionately impacting younger patients, given their longer life expectancy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
National Surgical Quality Improvement Program: What Can Anesthesiologists Learn From Surgical Outcomes?Anesth Analg. 2018 Jul;127(1):15-17. doi: 10.1213/ANE.0000000000003411. Anesth Analg. 2018. PMID: 29912055 No abstract available.
References
-
- Noordzij PG, Poldermans D, Schouten O, Bax JJ, Schreiner FA, Boersma E. Postoperative mortality in the Netherlands: a population-based analysis of surgery-specific risk in adults. Anesthesiology. 2010;112:1105–1115. - PubMed
-
- Pearse RM, Moreno RP, Bauer P, et al.; European Surgical Outcomes Study (EuSOS) group for the Trials groups of the European Society of Intensive Care Medicine and the European Society of Anaesthesiology.Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012;380:1059–1065. - PMC - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361:1368–1375. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
