

The obesity epidemic and rising diabetes incidence in a low-income racially diverse southern US cohort
- PMID: 29324894
- PMCID: PMC5764338
- DOI: 10.1371/journal.pone.0190993
The obesity epidemic and rising diabetes incidence in a low-income racially diverse southern US cohort
Abstract
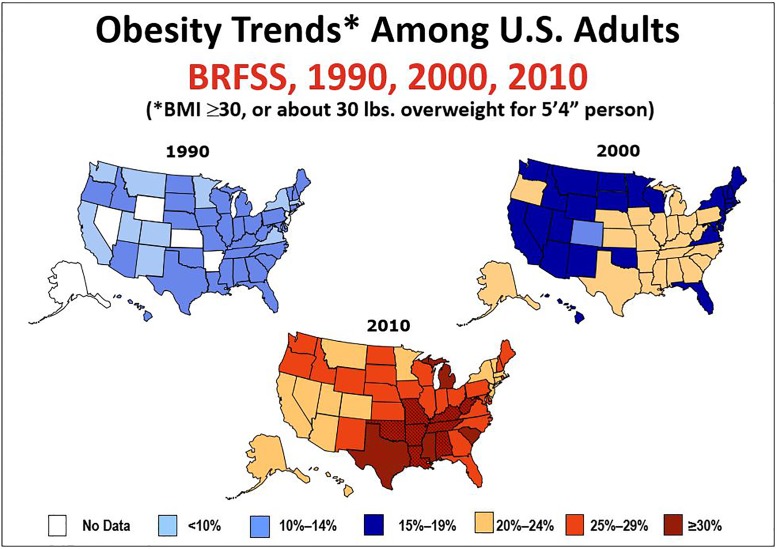
Background: Obesity is known to be a major risk factor for diabetes, but the magnitude of risk and variation between blacks and whites are less well documented in populations heavily affected by obesity. Herein we assess rates and risks of incident diabetes in a diverse southern population where obesity is common.
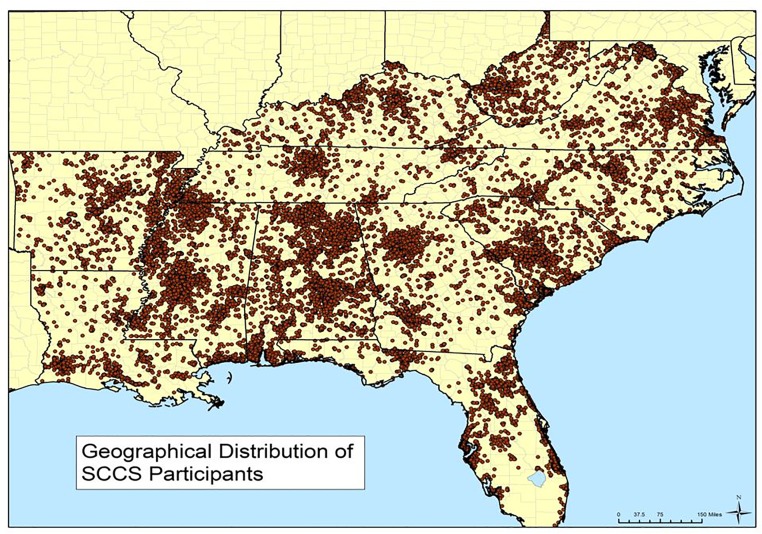
Methods: A total of 24,000 black and 14,064 white adults aged 40-79 in the Southern Community Cohort Study with no self-reported diabetes at study enrollment during 2002-2009 was followed for up to 10 (median 4.5) years. Incidence rates, odds ratios (OR) and accompanying 95% confidence intervals (CI) for medication-treated incident diabetes were determined according to body mass index (BMI) and other characteristics, including tobacco and alcohol consumption, healthy eating and physical activity indices, and socioeconomic status (SES).
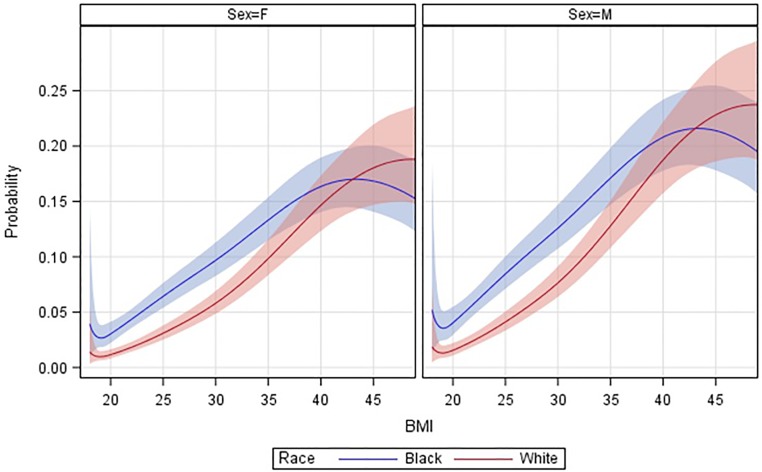
Results: Risk of incident diabetes rose monotonically with increasing BMI, but the trends differed between blacks and whites (pinteraction < .0001). Adjusted ORs (CIs) for diabetes among those with BMI≥40 vs 20-25 kg/m2 were 11.9 (8.4-16.8) for whites and 4.0 (3.3-4.8) for blacks. Diabetes incidence was more than twice as high among blacks than whites of normal BMI, but the racial difference became attenuated as BMI rose, with estimated 5-year probabilities of developing diabetes approaching 20% for both blacks and whites with BMI≥40 kg/m2. Diabetes risk was also associated with low SES, significantly (pinteraction≤.02) more so for whites, current cigarette smoking, and lower healthy eating and physical activity indices, although high BMI remained the predominant risk factor among both blacks and whites. From baseline prevalence and 20-year projections of the incidence trends, we estimate that the large majority of surviving cohort participants with BMI≥40 kg/m2 will be diagnosed with diabetes.
Conclusions: Even using conservative criteria to ascertain diabetes incidence (i.e., requiring diabetes medication use and ignoring undiagnosed cases), rates of obesity-associated diabetes were exceptionally high in this low-income adult population. The findings indicate that effective strategies to halt the rising prevalence of obesity are needed to avoid substantial increases in diabetes in coming years.
Conflict of interest statement
Figures
References
-
- Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL. Overweight and obesity in the United States: prevalence and trends, 1960–1994. Int J Obes Relat Metab Disord. 1998;22: 39–47. - PubMed
-
- Pi-Sunyer FX. The obesity epidemic: pathophysiology and consequences of obesity. Obes Res. 2002;10 Suppl 2: 97S–104S. doi: 10.1038/oby.2002.202 - DOI - PubMed
-
- Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315: 2284–2291. doi: 10.1001/jama.2016.6458 - DOI - PMC - PubMed
-
- Beydoun MA, Wang Y. Gender-ethnic disparity in BMI and waist circumference distribution shifts in US adults. Obesity (Silver Spring). 2009;17: 169–176. doi: 10.1038/oby.2008.492 - DOI - PMC - PubMed
-
- Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1998–2012. JAMA. 2015;314: 1021–1029. doi: 10.1001/jama.2015.10029 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
