

doi: 10.1093/cid/ciy011.
Urine Tuberculosis Lipoarabinomannan Predicts Mortality in Hospitalized Human Immunodeficiency Virus-Infected Children
Affiliations
- PMID: 29324985
- PMCID: PMC5961239
- DOI: 10.1093/cid/ciy011
Item in Clipboard
Urine Tuberculosis Lipoarabinomannan Predicts Mortality in Hospitalized Human Immunodeficiency Virus-Infected Children
Clin Infect Dis.
.
Abstract
Figures
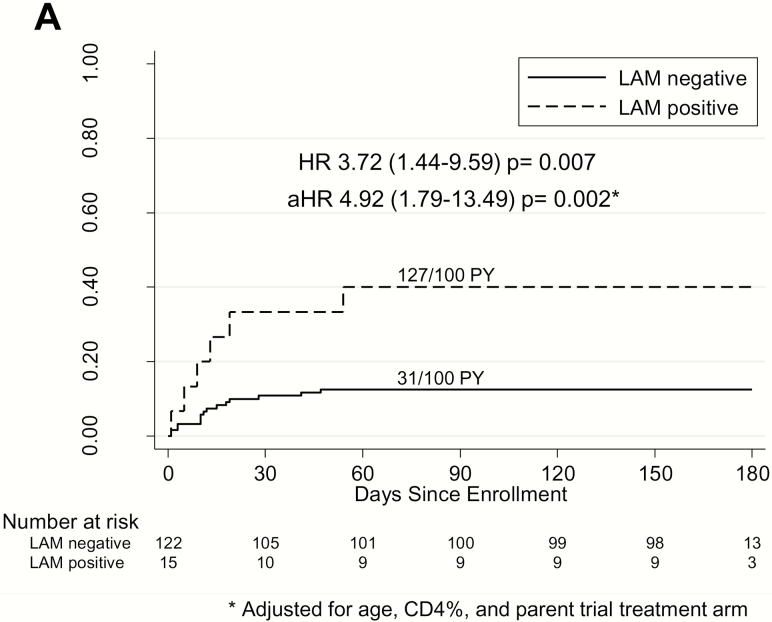
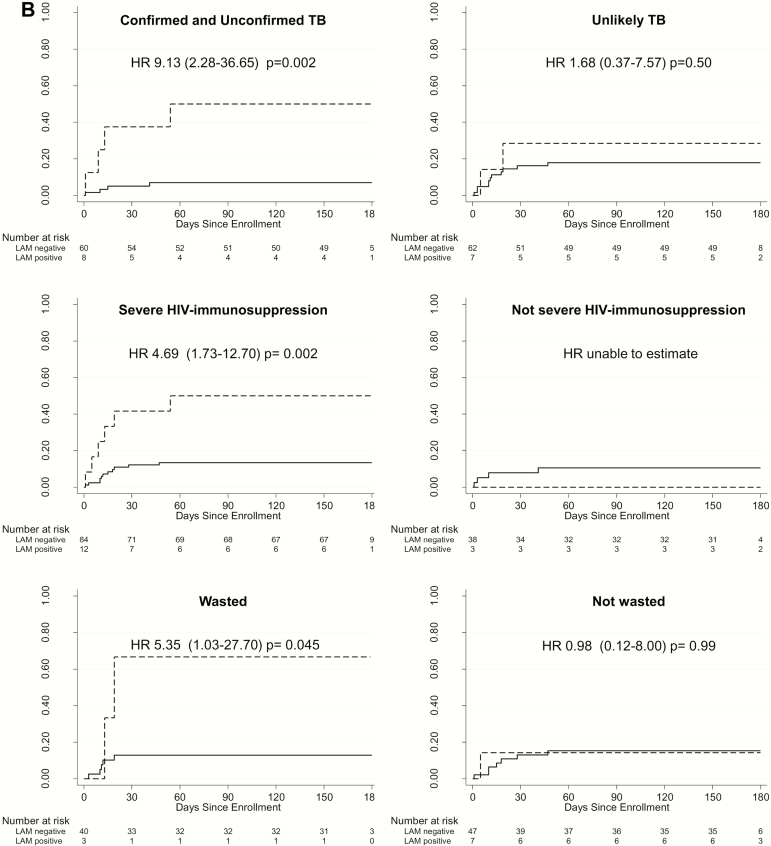
A, Cumulative probability of death by urine LAM result among hospitalized HIV–infected children. * indicates adjusted for age, CD4%, and parent trial antiretroviral therapy treatment arm. B, Cumulative probability of death by urine LAM result among hospitalized HIV-infected children stratified by TB, HIV-related immunosuppression, and malnutrition status. Confirmed TB was that for which a bacterial confirmation was obtained with positive respiratory sample Xpert or culture result. Unconfirmed TB was that for which bacterial confirmation was not obtained and at least 2 of the following were present: suggestive symptoms of TB, chest X-ray consistent with TB, close TB exposure or immunologic evidence of Mycobacterium tuberculosis infection, TB treatment response. Unlikely TB was that not fitting in any of the TB diagnosis criteria. (Graham et al [7]). Severe immunosuppression was based on World Health Organization (WHO) age-specified CD4 cutoffs—CD4%: aged <12 months, <25%; aged 12–35 months, <20%; aged >36 months, <15%—or, in absence of CD4% data, CD4 count: aged <12 months, <1500 cells/µL; aged 12–35 months, <750 cells/µL; aged >36 months, <350 cells/µL (WHO 2007). Malnourished was based on WHO definitions of wasting with either weight-to-height z score <−2 or mid–upper arm circumference <12.5 cm. Abbreviations: aHR, adjusted hazard ratio; HIV, human immunodeficiency virus; HR, hazard ratio; LAM, lipoarabinomannan; PY, person-years; TB, tuberculosis.
A, Cumulative probability of death by urine LAM result among hospitalized HIV–infected children. * indicates adjusted for age, CD4%, and parent trial antiretroviral therapy treatment arm. B, Cumulative probability of death by urine LAM result among hospitalized HIV-infected children stratified by TB, HIV-related immunosuppression, and malnutrition status. Confirmed TB was that for which a bacterial confirmation was obtained with positive respiratory sample Xpert or culture result. Unconfirmed TB was that for which bacterial confirmation was not obtained and at least 2 of the following were present: suggestive symptoms of TB, chest X-ray consistent with TB, close TB exposure or immunologic evidence of Mycobacterium tuberculosis infection, TB treatment response. Unlikely TB was that not fitting in any of the TB diagnosis criteria. (Graham et al [7]). Severe immunosuppression was based on World Health Organization (WHO) age-specified CD4 cutoffs—CD4%: aged <12 months, <25%; aged 12–35 months, <20%; aged >36 months, <15%—or, in absence of CD4% data, CD4 count: aged <12 months, <1500 cells/µL; aged 12–35 months, <750 cells/µL; aged >36 months, <350 cells/µL (WHO 2007). Malnourished was based on WHO definitions of wasting with either weight-to-height z score <−2 or mid–upper arm circumference <12.5 cm. Abbreviations: aHR, adjusted hazard ratio; HIV, human immunodeficiency virus; HR, hazard ratio; LAM, lipoarabinomannan; PY, person-years; TB, tuberculosis.
References
-
- World Health Organization. The use of lateral flow urine lipoarabinomannan assay (LF-LAM) for the diagnosis and screening of active tuberculosis in people living with HIV Available at: http://www.who.int/tb/publications/use-of-lf-lam-tb-hiv/en/. Accessed 21 September 2017.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
