

The Addition of Chemotherapy to Radiation Therapy Improves Survival in Elderly Patients with Stage III Non-Small Cell Lung Cancer
- PMID: 29326090
- PMCID: PMC5910031
- DOI: 10.1016/j.jtho.2017.11.135
The Addition of Chemotherapy to Radiation Therapy Improves Survival in Elderly Patients with Stage III Non-Small Cell Lung Cancer
Abstract
Introduction: Elderly patients account for the majority of lung cancer diagnoses but are poorly represented in clinical trials. We evaluated the overall survival (OS) of elderly patients with stage III NSCLC treated with definitive radiation compared with that of patients treated with definitive chemoradiation.
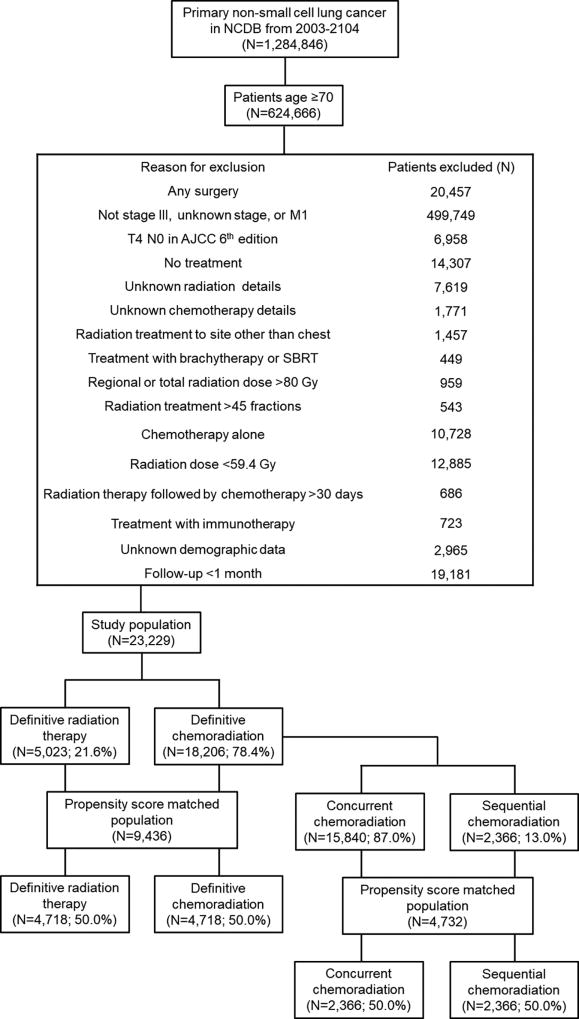
Methods: We conducted a comparative effectiveness study of radiation therapy versus chemoradiation in elderly (≥70 years old) patients with stage III NSCLC not treated surgically diagnosed from 2003 to 2014; the patients were identified by using the National Cancer Database. Two cohorts were evaluated: patients (n = 5023) treated with definitive radiation (≥59.4 Gy) and patients (n = 18,206) treated with definitive chemoradiation. Chemoradiation was further defined as concurrent (radiation and chemotherapy started within 30 days of each other) or sequential (radiation started >30 days after chemotherapy). We compared OS between the treatment groups by using the Kaplan-Meier method and Cox proportional hazards regression before and after propensity score matching (PSM).
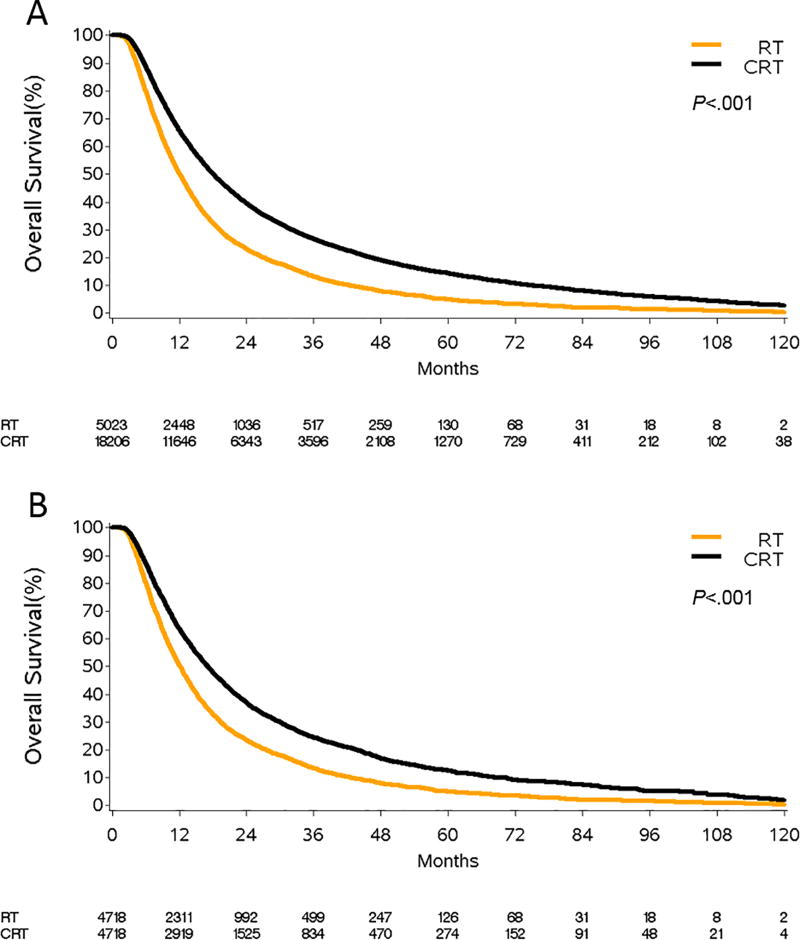
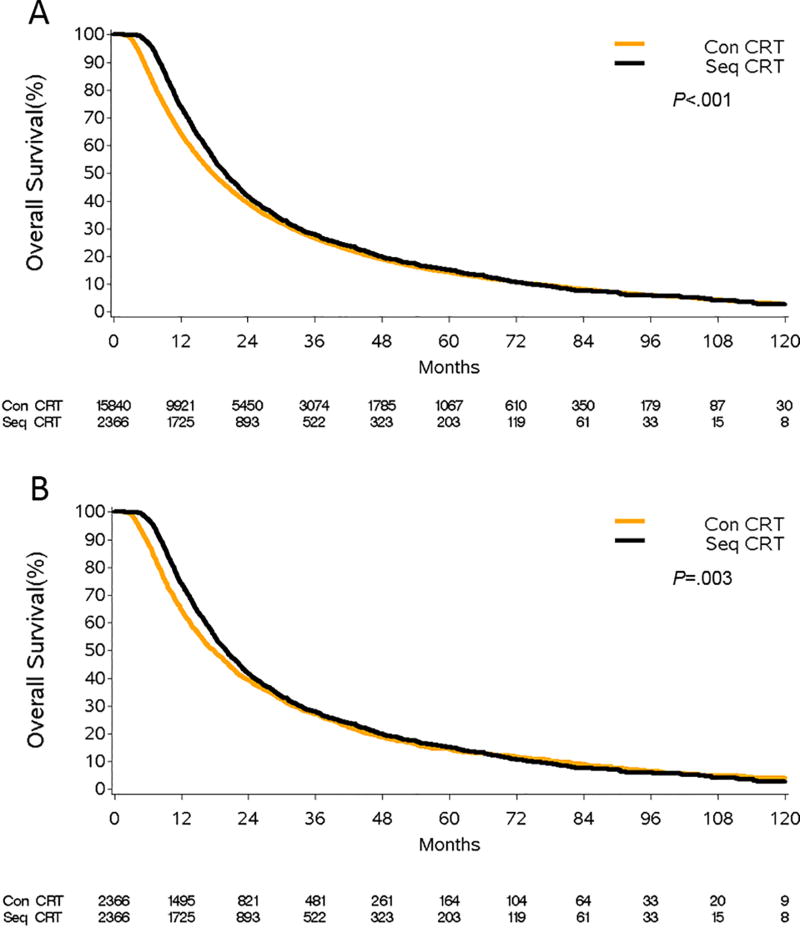
Results: Treatment with chemoradiation was associated with improved OS versus that with radiation both before PSM (hazard ratio [HR] = 0.66, 95% confidence interval [CI]: 0.64-0.68, p < 0.001) and after PSM (HR = 0.67, 95% CI: 0.64-0.70, p < 0.001). Relative to concurrent chemoradiation, sequential chemoradiation was associated with a 9% reduction in the risk for death (HR = 0.91, 95% CI: 0.85-0.96, p = 0.002).
Conclusions: We found that definitive chemoradiation resulted in a survival advantage compared with definitive radiation in elderly patients. Sequential chemotherapy and radiation was superior to concurrent chemoradiation. Although prospective trials are needed, this analysis suggests that chemoradiation should be strongly considered for elderly patients and the optimal sequencing of chemotherapy and radiation remains an unanswered question for this patient population.
Keywords: Chemotherapy; Elderly; Non–small cell; Radiation therapy; Stage III.
Copyright © 2017 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Authors’ Disclosures of Potential Conflicts of Interest: The authors have no conflicts of interest to disclose.
Figures
Comment in
-
Elderly patients with stage III NSCLC survive longer when chemotherapy is added to radiotherapy-fortune favours the bold.Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S388-S392. doi: 10.21037/tlcr.2018.08.12. Transl Lung Cancer Res. 2018. PMID: 30705864 Free PMC article. No abstract available.
References
-
- Crino L, Weder W, van Meerbeeck J, et al. Early stage and locally advanced (non-metastatic) non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v103–115. - PubMed
-
- National Cancer Institute. [Accessed June 13, 2017];SEER stat fact sheets: Lung and bronchus cancer. http://seer.Cancer.Gov/csr/1975_2014/
-
- Sacher AG, Le LW, Leighl NB, et al. Elderly patients with advanced NSCLC in phase III clinical trials: Are the elderly excluded from practice-changing trials in advanced NSCLC? J Thorac Oncol. 2013;8:366–368. - PubMed
-
- Langer CJ. Neglected and underrepresented subpopulations: Elderly and performance status 2 patients with advanced-stage non-small-cell lung cancer. Clin Lung Cancer. 2006;7(Suppl 4):S126–137. - PubMed
-
- Lewis JH, Kilgore ML, Goldman DP, et al. Participation of patients 65 years of age or older in cancer clinical trials. J Clin Oncol. 2003;21:1383–1389. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
