

Machine Learning Algorithm Predicts Cardiac Resynchronization Therapy Outcomes: Lessons From the COMPANION Trial
- PMID: 29326129
- PMCID: PMC5769699
- DOI: 10.1161/CIRCEP.117.005499
Machine Learning Algorithm Predicts Cardiac Resynchronization Therapy Outcomes: Lessons From the COMPANION Trial
Abstract
Background: Cardiac resynchronization therapy (CRT) reduces morbidity and mortality in heart failure patients with reduced left ventricular function and intraventricular conduction delay. However, individual outcomes vary significantly. This study sought to use a machine learning algorithm to develop a model to predict outcomes after CRT.
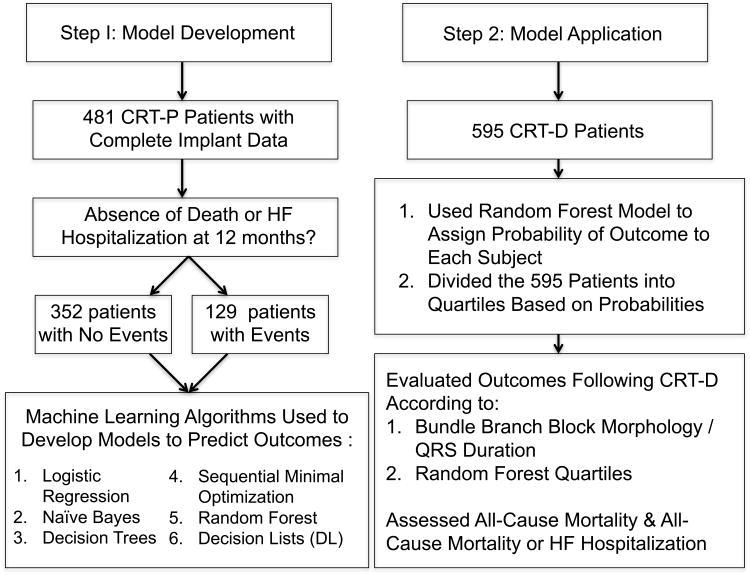
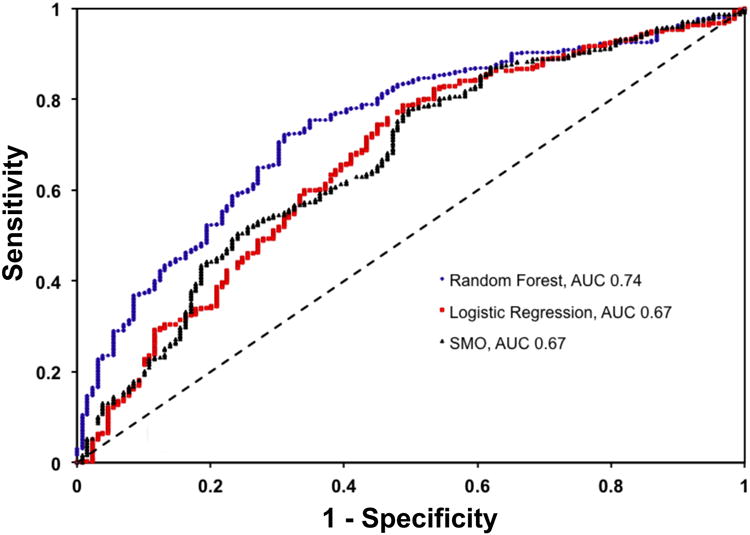
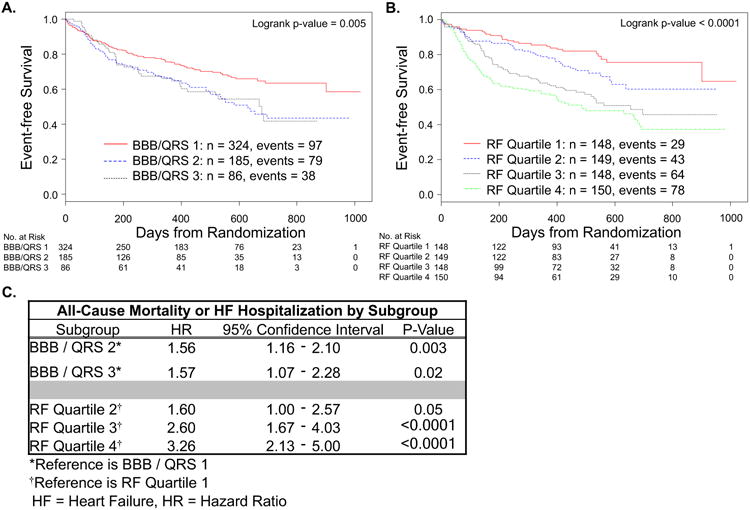
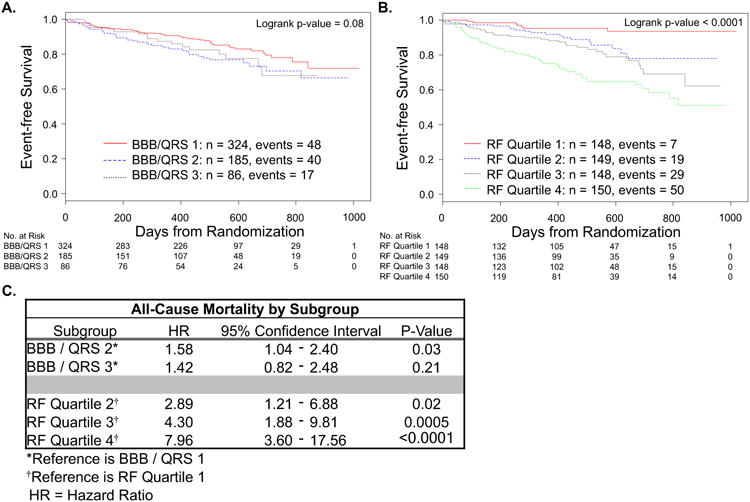
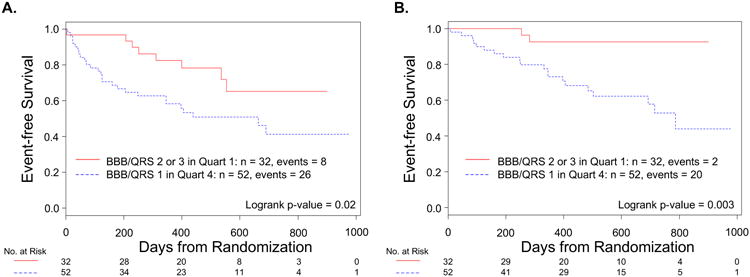
Methods and results: Models were developed with machine learning algorithms to predict all-cause mortality or heart failure hospitalization at 12 months post-CRT in the COMPANION trial (Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure). The best performing model was developed with the random forest algorithm. The ability of this model to predict all-cause mortality or heart failure hospitalization and all-cause mortality alone was compared with discrimination obtained using a combination of bundle branch block morphology and QRS duration. In the 595 patients with CRT-defibrillator in the COMPANION trial, 105 deaths occurred (median follow-up, 15.7 months). The survival difference across subgroups differentiated by bundle branch block morphology and QRS duration did not reach significance (P=0.08). The random forest model produced quartiles of patients with an 8-fold difference in survival between those with the highest and lowest predicted probability for events (hazard ratio, 7.96; P<0.0001). The model also discriminated the risk of the composite end point of all-cause mortality or heart failure hospitalization better than subgroups based on bundle branch block morphology and QRS duration.
Conclusions: In the COMPANION trial, a machine learning algorithm produced a model that predicted clinical outcomes after CRT. Applied before device implant, this model may better differentiate outcomes over current clinical discriminators and improve shared decision-making with patients.
Keywords: algorithms; cardiac resynchronization therapy; heart failure; hospitalization; machine learning.
© 2018 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
Computer Modeling: The Future of Cardiac Resynchronization Therapy Patient Selection?Circ Arrhythm Electrophysiol. 2018 Jan;11(1):e006104. doi: 10.1161/CIRCEP.117.006104. Circ Arrhythm Electrophysiol. 2018. PMID: 29326131 No abstract available.
References
-
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NM, III, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329–1338. - PubMed
-
- Tang AS, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, Hohnloser SH, Nichol G, Birnie DH, Sapp JL, Yee R, Healey JS, Rouleau JL. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010;363:2385–2395. - PubMed
-
- Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52:1834–1843. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
