

Weekly Standard Kt/Vurea and Clinical Outcomes in Home and In-Center Hemodialysis
- PMID: 29326306
- PMCID: PMC5967669
- DOI: 10.2215/CJN.05680517
Weekly Standard Kt/Vurea and Clinical Outcomes in Home and In-Center Hemodialysis
Abstract
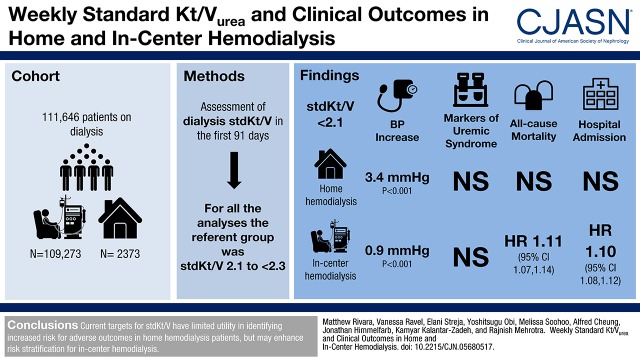
Background and objectives: Patients undergoing hemodialysis with a frequency other than thrice weekly are not included in current clinical performance metrics for dialysis adequacy. The weekly standard Kt/Vurea incorporates treatment frequency, but there are limited data on its association with clinical outcomes.
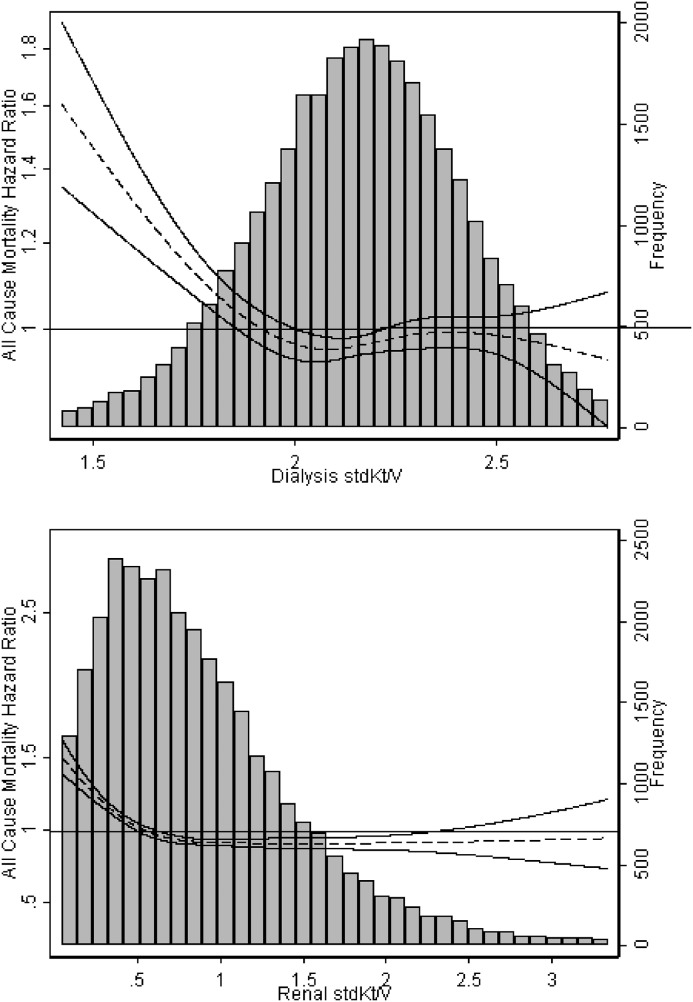
Design, setting, participants, & measurements: We used multivariable regression to examine the association of dialysis standard Kt/Vurea with BP and metabolic control (serum potassium, calcium, bicarbonate, and phosphorus) in patients incidental to dialysis treated with home (n=2373) or in-center hemodialysis (n=109,273). We further used Cox survival models to examine the association of dialysis standard Kt/Vurea with mortality, hospitalization, and among patients on home hemodialysis, transfer to in-center hemodialysis.
Results: After adjustment for potential confounders, patients with dialysis standard Kt/Vurea <2.1 had higher BPs compared with patients with standard Kt/Vurea 2.1 to <2.3 (3.4 mm Hg higher [P<0.001] for home hemodialysis and 0.9 mm Hg higher [P<0.001] for in-center hemodialysis). There were no clinically meaningful associations between dialysis standard Kt/Vurea and markers of metabolic control, irrespective of dialysis modality. There was no association between dialysis standard Kt/Vurea and risk for mortality, hospitalization, or transfer to in-center hemodialysis among patients undergoing home hemodialysis. Among patients on in-center hemodialysis, dialysis standard Kt/Vurea <2.1 was associated with higher risk (adjusted hazard ratio, 1.11; 95% confidence interval, 1.07 to 1.14) and standard Kt/Vurea ≥2.3 was associated with lower risk (adjusted hazard ratio, 0.97; 95% confidence interval, 0.94 to 0.99) for death compared with standard Kt/Vurea 2.1 to <2.3. Additional analyses limited to patients with available data on residual kidney function showed similar relationships of dialysis and total (dialysis plus kidney) standard Kt/Vurea with outcomes.
Conclusions: Current targets for standard Kt/Vurea have limited utility in identifying individuals at increased risk for adverse clinical outcomes for those undergoing home hemodialysis but may enhance risk stratification for in-center hemodialysis.
Keywords: Bicarbonates; Blood Pressure Determination; Confidence Intervals; Epidemiology and outcomes; Hemodialysis, Home; Odds Ratio; Phosphorus; Potassium; Risk; blood pressure; calcium bicarbonate; hemodialysis adequacy; hospitalization; mortality risk; renal dialysis.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- United States Renal Data System : USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2016
-
- Centers for Medicare & Medicaid Services (CMS) ; HHS: Medicare program; end-stage renal disease prospective payment system, and quality incentive program. Final rule. Fed Regist 80: 68968–69077, 2015 - PubMed
-
- Eknoyan G, Beck GJ, Cheung AK, Daugirdas JT, Greene T, Kusek JW, Allon M, Bailey J, Delmez JA, Depner TA, Dwyer JT, Levey AS, Levin NW, Milford E, Ornt DB, Rocco MV, Schulman G, Schwab SJ, Teehan BP, Toto R; Hemodialysis (HEMO) Study Group : Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med 347: 2010–2019, 2002 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
