

The different faces of renal angiomyolipomas on radiologic imaging: a pictorial review
- PMID: 29327940
- PMCID: PMC5965995
- DOI: 10.1259/bjr.20170533
The different faces of renal angiomyolipomas on radiologic imaging: a pictorial review
Abstract
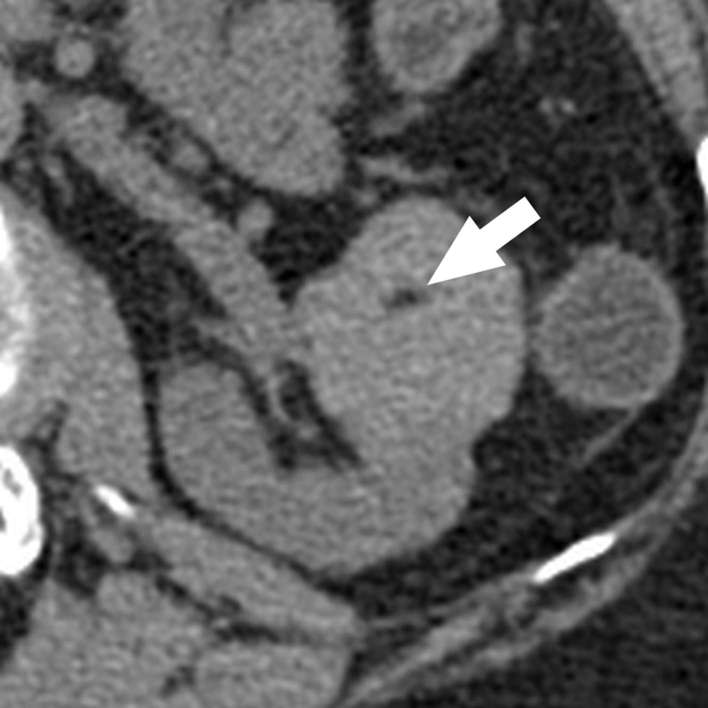
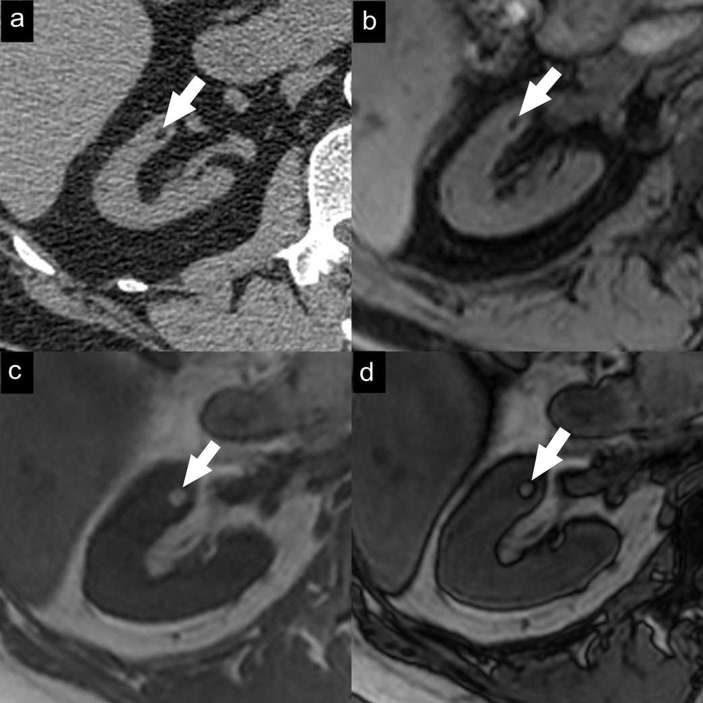
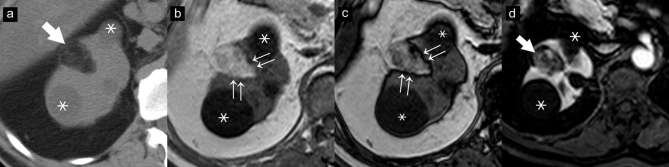
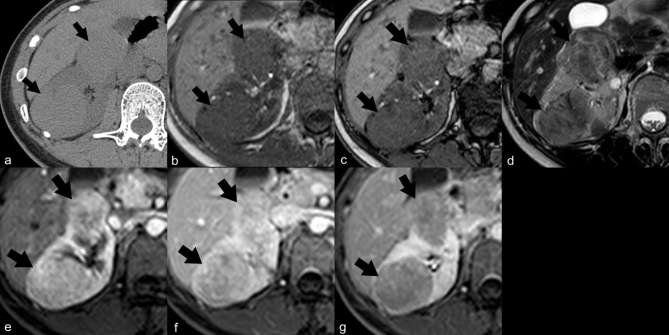
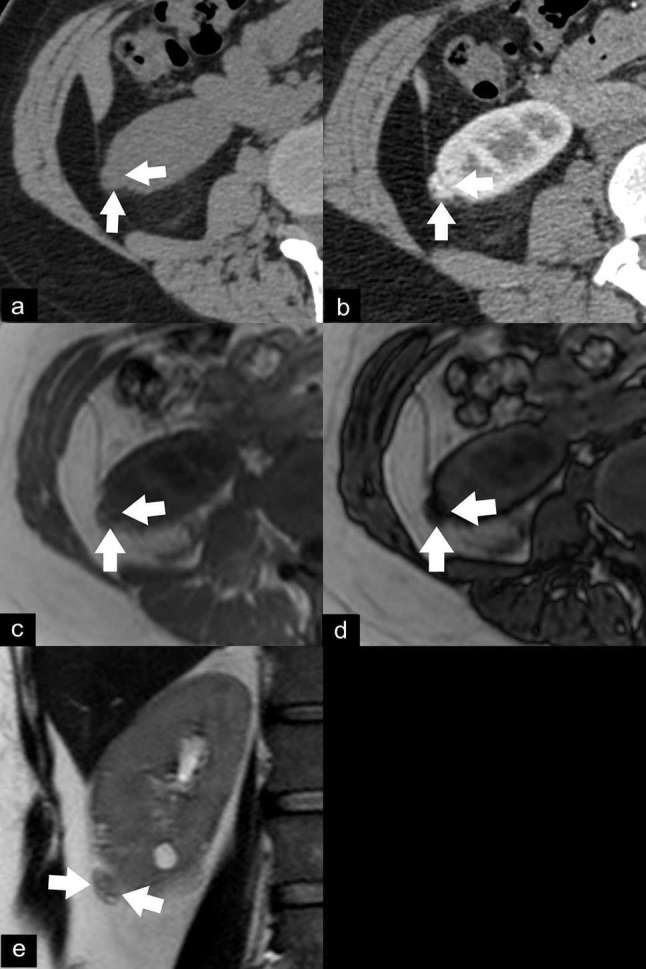
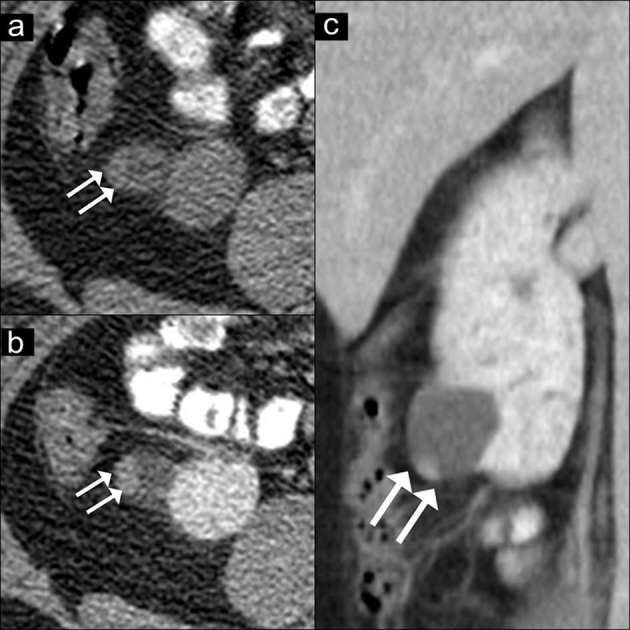
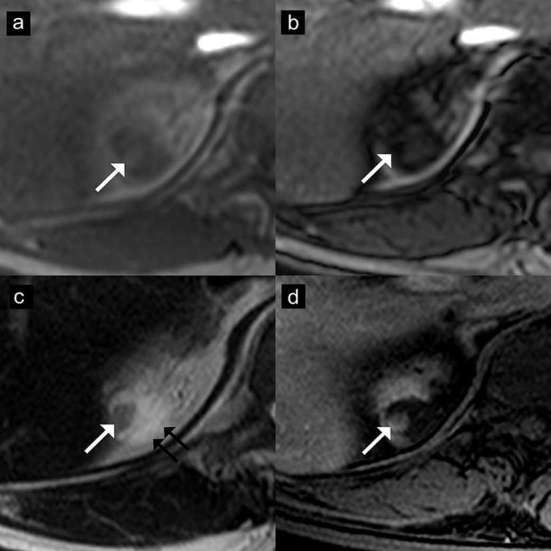
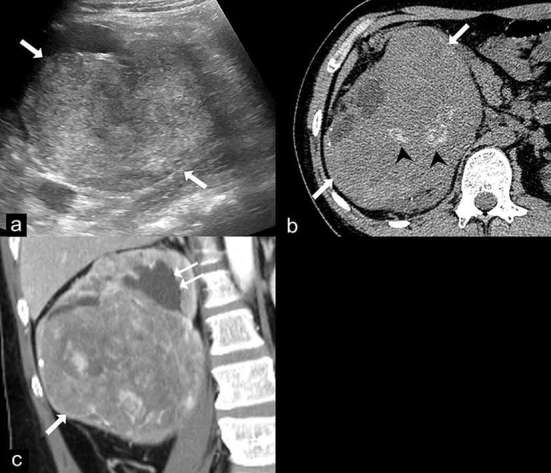
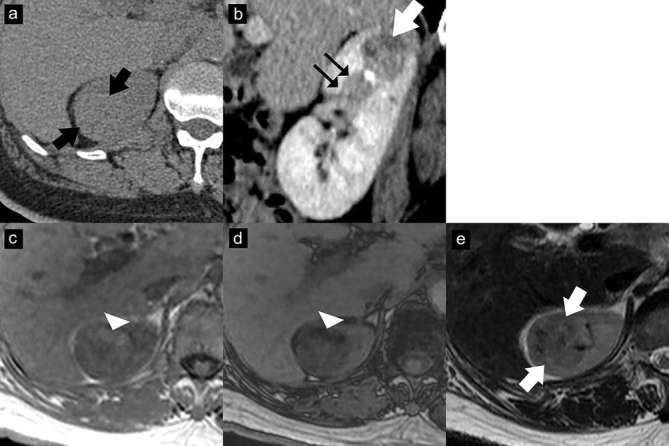
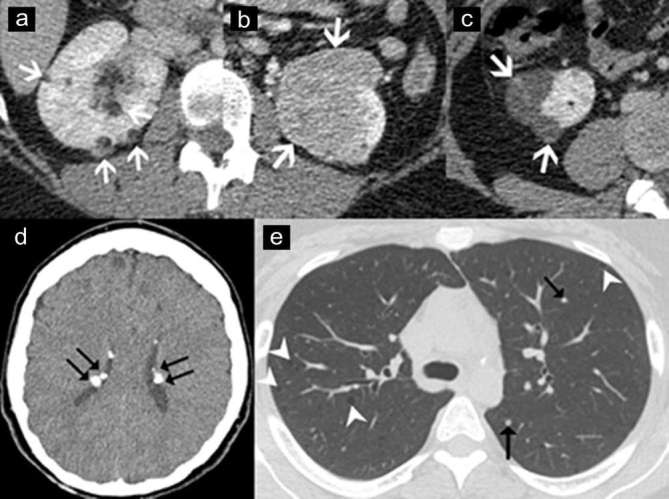
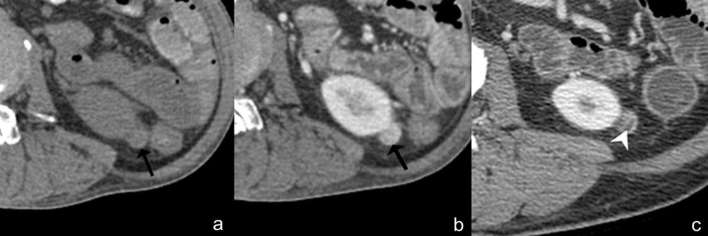
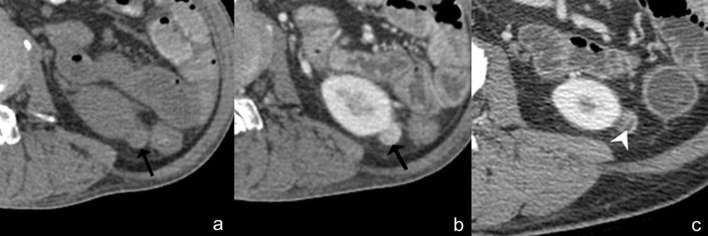
Renal angiomyolipoma (AML) is an uncommon renal tumour, generally composed of mature adipose tissue, dysmorphic blood vessels and smooth muscle. Identification of intratumoral fat on unenhanced CT images is the most reliable finding for establishing the diagnosis of renal AML. However, AMLs sometimes exhibit atypical findings, including cystic as well as solid forms; some of these variants overlap with the appearance of other renal tumours. A rare type of AML, the epithelioid type, possesses malignant potential. The aim of this pictorial review is to gather the different imaging features of AMLs including the classic and fat-poor types, AMLs with epithelial cysts, epithelioid AML, AML associated with tuberous sclerosis, haemorrhagic AML and large AMLs mimicking retroperitoneal liposarcomas. The diagnostic clues that help to distinguish AMLs from other renal tumours are also described in the review.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
