

Consequence of intraventricular hemorrhage on neurovascular coupling evoked by speech syllables in preterm neonates
- PMID: 29328980
- PMCID: PMC6969131
- DOI: 10.1016/j.dcn.2018.01.001
Consequence of intraventricular hemorrhage on neurovascular coupling evoked by speech syllables in preterm neonates
Abstract
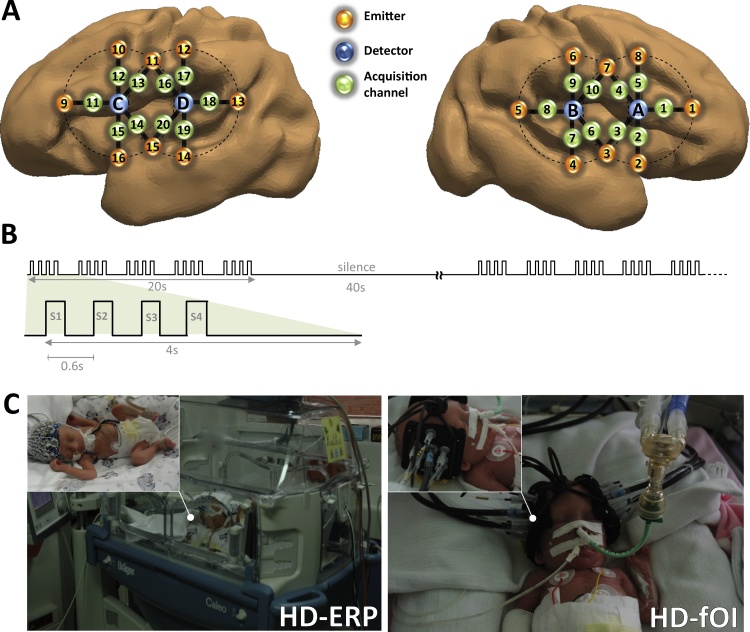
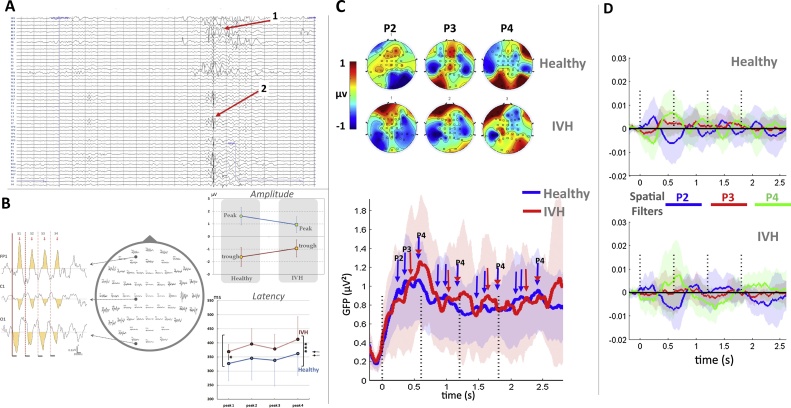
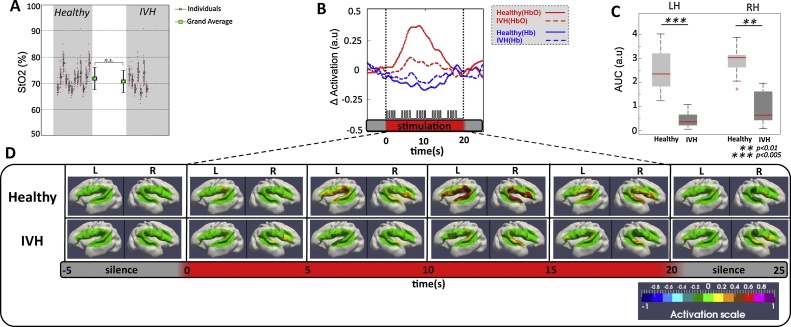
Intraventricular Hemorrhage (IVH) is the leading cause of neurological and cognitive impairment in preterm neonates with an incidence that increases with increasing prematurity. In the present study, we tested how preterm neonates with IVH react to external stimulation (i.e. speech syllables). We compared their neural responses measured by electroencephalography (EEG), and hemodynamic responses measured by functional near-infrared spectroscopy (fNIRS), with those of healthy preterms. A neural response to syllables was observed in these infants, but did not induce a vascular response in contrast with healthy neonates. These results clearly demonstrate that the cerebral vascular network in IVH preterm neonates was unable to compensate for the increased metabolism resulting from neuronal activation in response to external stimulation. Optical imaging is thus a sensitive tool to identify altered cerebral hemodynamic in critically ill preterms before behavioral changes are manifested or when only minor abnormalities on other functional monitoring techniques such as EEG are visible. We propose that a multi-modal approach provides unique opportunities for early monitoring of cognitive functions and opens up new possibilities for clinical care and recommended practices by studying the difficulties of the premature brain to adapt to its environment.
Keywords: Electroencephalogram (EEG); Functional Near Infrared Spectroscopy (fNIRS); Intraventricular hemorrhage; Neurovascular coupling; Preterm.
Copyright © 2018 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Alderliesten T., Lemmers P.M., Smarius J.J., van de Vosse R.E., Baerts W., van Bel F. Cerebral oxygenation, extraction, and autoregulation in very preterm infants who develop peri-intraventricular hemorrhage. J. Pediatr. 2013;162:698–704. e692. - PubMed
-
- Ardila A., Ostrosky-Solis F. Gordon and Breach; 1984. The Right Hemisphere: Neurology and Neuropsychology.
-
- Bartocci M., Bergqvist L.L., Lagercrantz H., Anand K.J. Pain activates cortical areas in the preterm newborn brain. Pain. 2006;122:109–117. - PubMed
-
- Bisiacchi P.S., Mento G., Suppiej A. Cortical auditory processing in preterm newborns: an ERP study. Biol. Psychol. 2009;82:176–185. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
