

Transcriptomic evidence of immune activation in macroscopically normal-appearing and scarred lung tissues in idiopathic pulmonary fibrosis
- PMID: 29329637
- PMCID: PMC5826809
- DOI: 10.1016/j.cellimm.2018.01.002
Transcriptomic evidence of immune activation in macroscopically normal-appearing and scarred lung tissues in idiopathic pulmonary fibrosis
Abstract
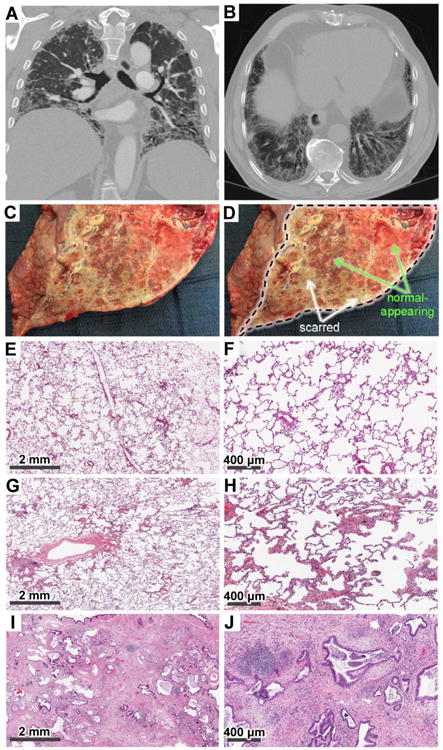
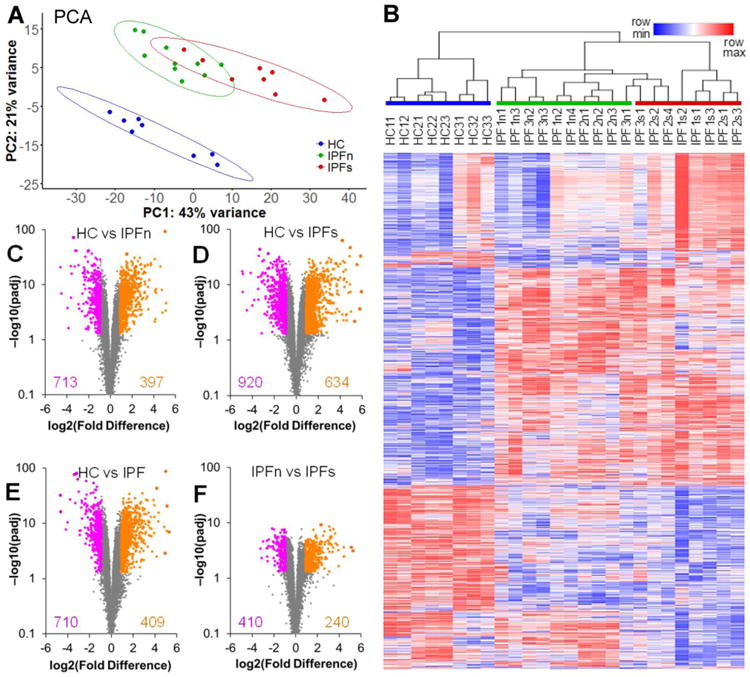
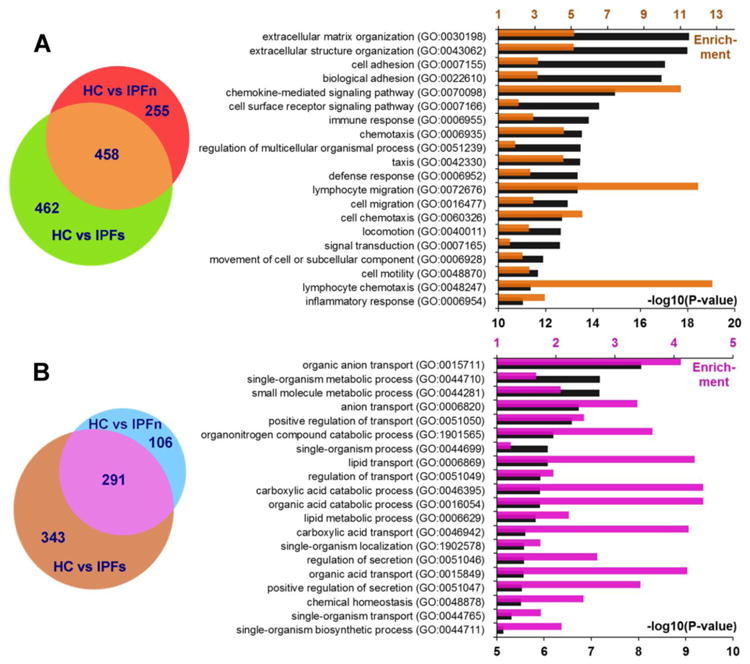
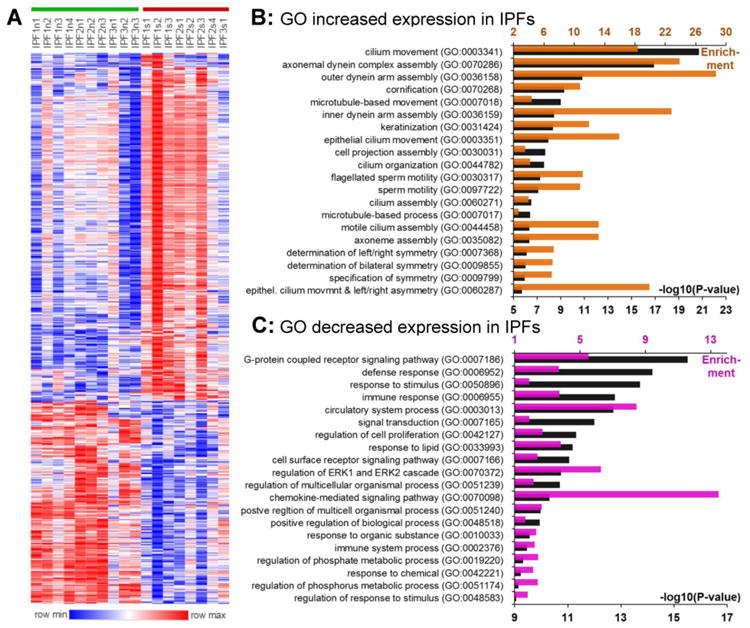
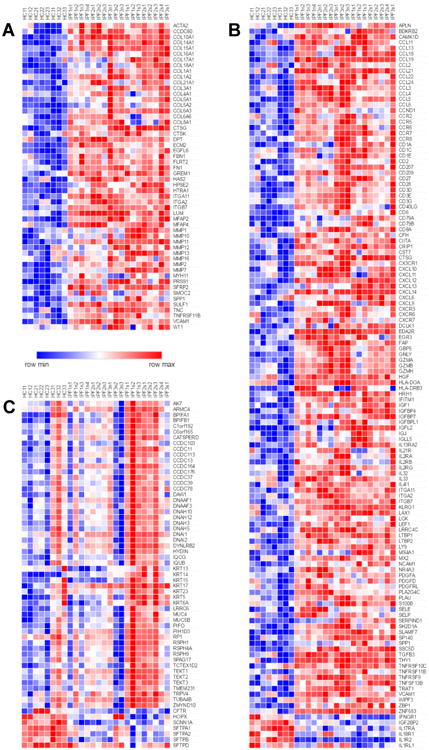
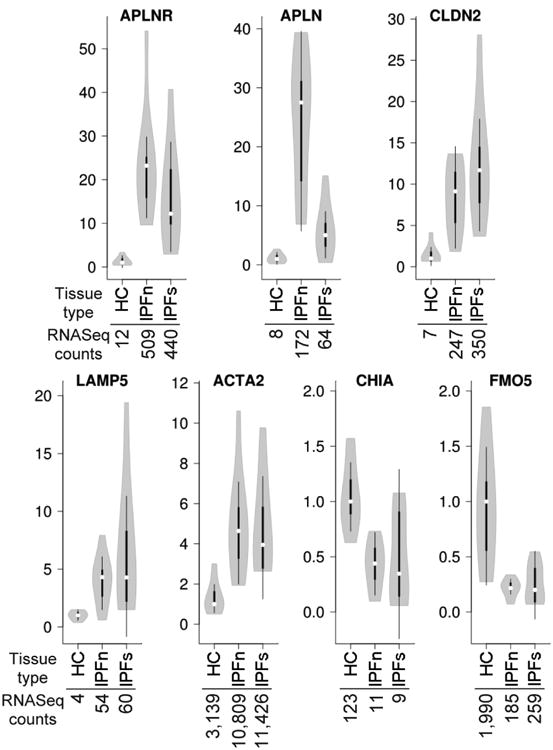
Idiopathic pulmonary fibrosis (IPF) is a fatal lung disease manifested by overtly scarred peripheral and basilar regions and more normal-appearing central lung areas. Lung tissues from macroscopically normal-appearing (IPFn) and scarred (IPFs) areas of explanted IPF lungs were analyzed by RNASeq and compared with healthy control (HC) lung tissues. There were profound transcriptomic changes in IPFn compared with HC tissues, which included elevated expression of numerous immune-, inflammation-, and extracellular matrix-related mRNAs, and these changes were similar to those observed with IPFs compared to HC. Comparing IPFn directly to IPFs, elevated expression of epithelial mucociliary mRNAs was observed in the IPFs tissues. Thus, despite the known geographic tissue heterogeneity in IPF, the entire lung is actively involved in the disease process, and demonstrates pronounced elevated expression of numerous immune-related genes. Differences between normal-appearing and scarred tissues may thus be driven by deranged epithelial homeostasis or possibly non-transcriptomic factors.
Keywords: Fibrosis; Inflammation; Lung; Transcriptome.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Bradley B, Branley HM, Egan JJ, Greaves MS, Hansell DM, Harrison NK, Hirani N, Hubbard R, Lake F, Millar AB, Wallace WA, Wells AU, Whyte MK, Wilsher ML B.T.S.S.o.C.C. British Thoracic Society Interstitial Lung Disease Guideline Group, A. Thoracic Society of, S. New Zealand Thoracic, S. Irish Thoracic. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63(5):v1–58. - PubMed
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, Lynch DA, Ryu JH, Swigris JJ, Wells AU, Ancochea J, Bouros D, Carvalho C, Costabel U, Ebina M, Hansell DM, Johkoh T, Kim DS, King TE, Jr, Kondoh Y, Myers J, Muller NL, Nicholson AG, Richeldi L, Selman M, Dudden RF, Griss BS, Protzko SL, Schunemann HJ A.E.J.A.C.o.I.P. Fibrosis. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. American journal of respiratory and critical care medicine. 2011;183:788–824. - PMC - PubMed
-
- Travis WD, Costabel U, Hansell DM, King TE, Jr, Lynch DA, Nicholson AG, Ryerson CJ, Ryu JH, Selman M, Wells AU, Behr J, Bouros D, Brown KK, Colby TV, Collard HR, Cordeiro CR, Cottin V, Crestani B, Drent M, Dudden RF, Egan J, Flaherty K, Hogaboam C, Inoue Y, Johkoh T, Kim DS, Kitaichi M, Loyd J, Martinez FJ, Myers J, Protzko S, Raghu G, Richeldi L, Sverzellati N, Swigris J, Valeyre D A.E.C.o.I.I. Pneumonias. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. American journal of respiratory and critical care medicine. 2013;188:733–748. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
