

Nasopharyngeal Lactobacillus is associated with a reduced risk of childhood wheezing illnesses following acute respiratory syncytial virus infection in infancy
- PMID: 29330010
- PMCID: PMC6039278
- DOI: 10.1016/j.jaci.2017.10.049
Nasopharyngeal Lactobacillus is associated with a reduced risk of childhood wheezing illnesses following acute respiratory syncytial virus infection in infancy
Abstract
Background: Early life acute respiratory infection (ARI) with respiratory syncytial virus (RSV) has been strongly associated with the development of childhood wheezing illnesses, but the pathways underlying this association are poorly understood.
Objective: To examine the role of the nasopharyngeal microbiome in the development of childhood wheezing illnesses following RSV ARI in infancy.
Methods: We conducted a nested cohort study of 118 previously healthy, term infants with confirmed RSV ARI by RT-PCR. We used next-generation sequencing of the V4 region of the 16S ribosomal RNA gene to characterize the nasopharyngeal microbiome during RSV ARI. Our main outcome of interest was 2-year subsequent wheeze.
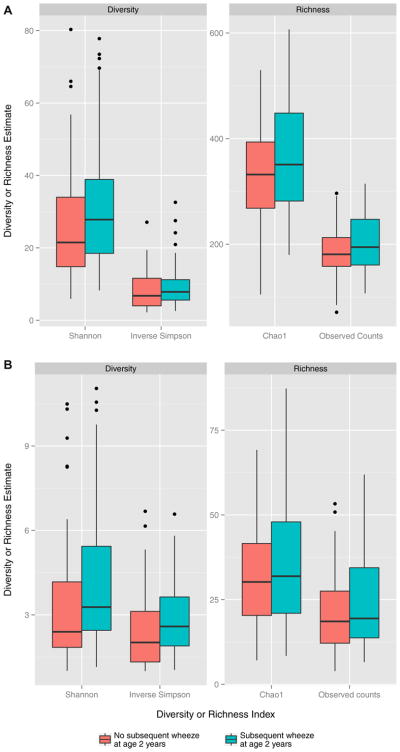
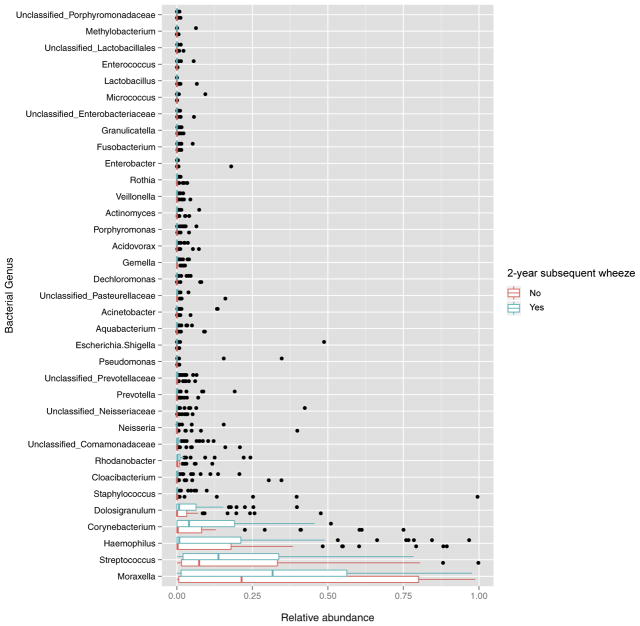
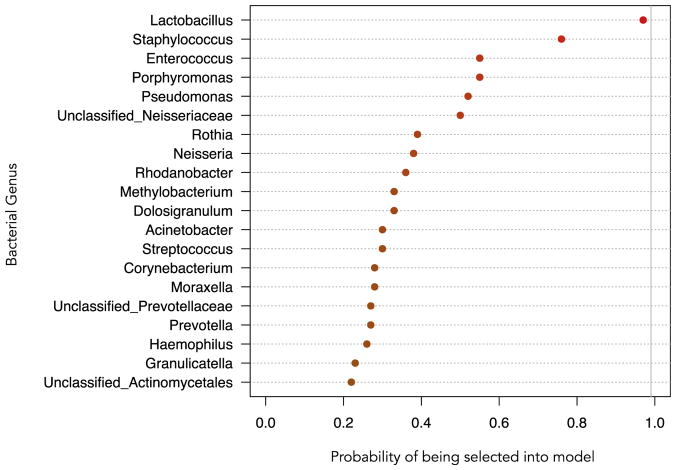
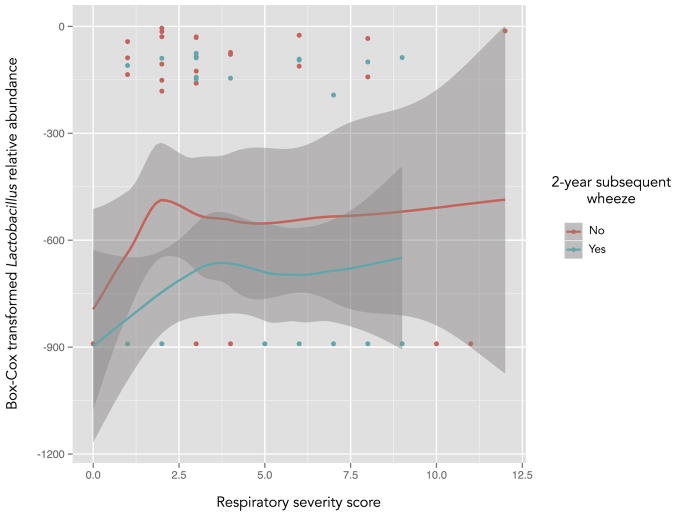
Results: Of the 118 infants, 113 (95.8%) had 2-year outcome data. Of these, 46 (40.7%) had parental report of subsequent wheeze. There was no association between the overall taxonomic composition, diversity, and richness of the nasopharyngeal microbiome during RSV ARI with the development of subsequent wheeze. However, the nasopharyngeal detection and abundance of Lactobacillus was consistently higher in infants who did not develop this outcome. Lactobacillus also ranked first among the different genera in a model distinguishing infants with and without subsequent wheeze.
Conclusions: The nasopharyngeal detection and increased abundance of Lactobacillus during RSV ARI in infancy are associated with a reduced risk of childhood wheezing illnesses at age 2 years.
Keywords: 16S ribosomal RNA sequencing; Lactobacillus; Microbiome; Staphylococcus; asthma; infants; nasopharynx; respiratory syncytial virus; wheezing.
Copyright © 2018 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure of potential conflict of interest: C. Rosas-Salazar has received a grant from the Francis Family Foundation. M. Shilts has received a grant and travel support from the National Institutes of Health. A. Tovchigrechko has received grants from J. Craig Venter Institute and the National Institutes of Health and is employed by and receives stock/stock options from MedImmune LLC. S. Schobel has received a grant from the J. Craig Venter Institute and the National Institutes of Health and is employed by the Henry M. Jackson Foundation. J. Chappell has received a grant from the National Institutes of Health. M. Moore has received a grant from the National Institutes of Health and is the founder of Meissa Vaccines. R. Peebles has received a grant from the National Institutes of Health. S. Das has received grants from the National Institutes of Health, Emergent Biosolution, Cargill, Abviro, and the Centers for Disease Control and is employed by Vanderbilt University Medical Center. T. Hartert has received grants from the National Institutes of Health and the Agency for Healthcare Research and Quality and is Associate Editor for the American Journal of Respiratory and Critical Care Medicine. The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Hall CB, Weinberg GA, Blumkin AK, Edwards KM, Staat MA, Schultz AF, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. 2013;132:e341–8. - PubMed
-
- Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiolitis-associated hospitalizations among US children, 1980–1996. JAMA. 1999;282:1440–6. - PubMed
-
- Stockman LJ, Curns AT, Anderson LJ, Fischer-Langley G. Respiratory syncytial virus-associated hospitalizations among infants and young children in the United States, 1997–2006. Pediatr Infect Dis J. 2012;31:5–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
