

Neuroendocrine Tumor Heterogeneity Adds Uncertainty to the World Health Organization 2010 Classification: Real-World Data from the Spanish Tumor Registry (R-GETNE)
- PMID: 29330208
- PMCID: PMC5896708
- DOI: 10.1634/theoncologist.2017-0364
Neuroendocrine Tumor Heterogeneity Adds Uncertainty to the World Health Organization 2010 Classification: Real-World Data from the Spanish Tumor Registry (R-GETNE)
Abstract
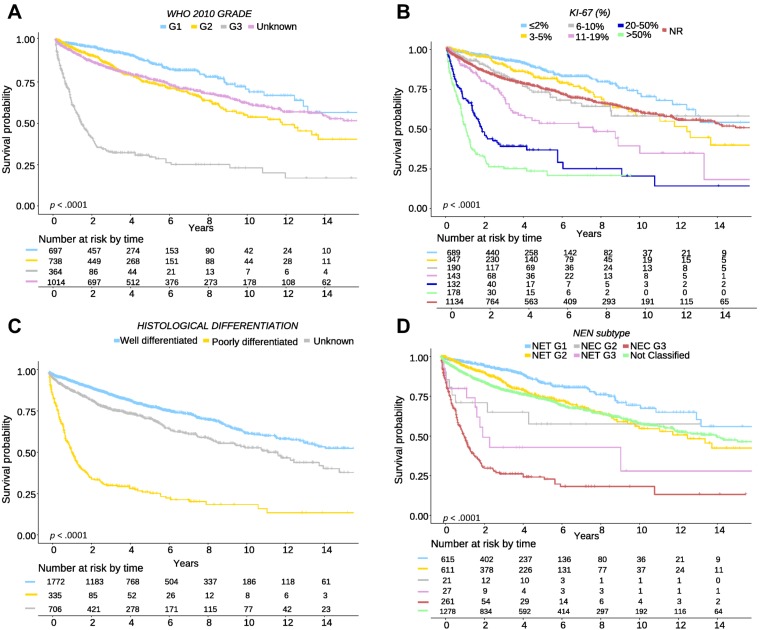
Background: Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs) are a complex family of tumors of widely variable clinical behavior. The World Health Organization (WHO) 2010 classification provided a valuable tool to stratify neuroendocrine neoplasms (NENs) in three prognostic subgroups based on the proliferation index. However, substantial heterogeneity remains within these subgroups, and simplicity sometimes entails an ambiguous and imprecise prognostic stratification. The purpose of our study was to evaluate the prognostic impact of histological differentiation within the WHO 2010 grade (G) 1/G2/G3 categories, and explore additional Ki-67 cutoff values in GEP-NENs.
Subjects, materials, and methods: A total of 2,813 patients from the Spanish National Tumor Registry (RGETNE) were analyzed. Cases were classified by histological differentiation as NETs (neuroendocrine tumors [well differentiated]) or NECs (neuroendocrine carcinomas [poorly differentiated]), and by Ki-67 index as G1 (Ki-67 <2%), G2 (Ki-67 3%-20%), or G3 (Ki-67 >20%). Patients were stratified into five cohorts: NET-G1, NET-G2, NET-G3, NEC-G2, and NEC-G3.
Results: Five-year survival was 72%. Age, gender, tumor site, grade, differentiation, and stage were all independent prognostic factors for survival. Further subdivision of the WHO 2010 grading improved prognostic stratification, both within G2 (5-year survival: 81% [Ki-67 3%-5%], 72% [Ki-67 6%-10%], 52% [Ki-67 11%-20%]) and G3 NENs (5-year survival: 35% [Ki-67 21%-50%], 22% [Ki-67 51%-100%]). Five-year survival was significantly greater for NET-G2 versus NEC-G2 (75.5% vs. 58.2%) and NET-G3 versus NEC-G3 (43.7% vs. 25.4%).
Conclusion: Substantial clinical heterogeneity is observed within G2 and G3 GEP-NENs. The WHO 2010 classification can be improved by including the additive effect of histological differentiation and the proliferation index.
Implications for practice: Gastroenteropancreatic neuroendocrine neoplasms are tumors of widely variable clinical behavior, roughly stratified by the World Health Organization (WHO) 2010 classification into three subgroups based on proliferation index. Real-world data from 2,813 patients of the Spanish Registry RGETNE demonstrated substantial clinical heterogeneity within grade (G) 2 and G3 neuroendocrine neoplasms. Tumor morphology and further subdivision of grading substantially improves prognostic stratification of these patients and may help individualize therapy. This combined, additive effect shall be considered in future classifications of neuroendocrine tumors and incorporated for stratification purposes in clinical trials.
Keywords: Gastroenteropancreatic; Heterogeneity; Ki‐67; Neuroendocrine neoplasms; Prognosis; Registry; Tumor differentiation; World Health Organization 2010.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Williams ED, Sandler M. The classification of carcinoid tumours. Lancet 1963;1:238–239. - PubMed
-
- Klöppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: The WHO classification. Ann N Y Acad Sci 2004;1014:13–27. - PubMed
-
- Rindi G, Arnold R, Bosman F et al. Nomenclature and classification of digestive neuroendocrine tumours In: Bosman FT, Carneiro F, Hruban R. et al., eds. WHO Classification of Tumours, Pathology and Genetics of Tumours of the Digestive System. 4th ed Lyon, France: International Agency for Research on Cancer (IARC) Press, 2010:10–12.
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
