

Multidimensional endotypes of chronic rhinosinusitis and their association with treatment outcomes
- PMID: 29331025
- PMCID: PMC6019131
- DOI: 10.1111/all.13411
Multidimensional endotypes of chronic rhinosinusitis and their association with treatment outcomes
Abstract
Background: The expression of chronic rhinosinusitis (CRS) is multidimensional. Disease heterogeneity in patients with CRS remains poorly understood. This study aimed to identify endotypes of CRS using cluster analysis by integrating multidimensional characteristics and to explore their association with treatment outcomes.
Methods: A total of 28 clinical variables and 39 mucosal cellular and molecular variables were analyzed using principal component analysis. Cluster analysis was performed on 246 prospectively recruited Chinese CRS patients with at least 1-year postoperative follow-up. Difficult-to-treat CRS was characterized in each generated cluster.
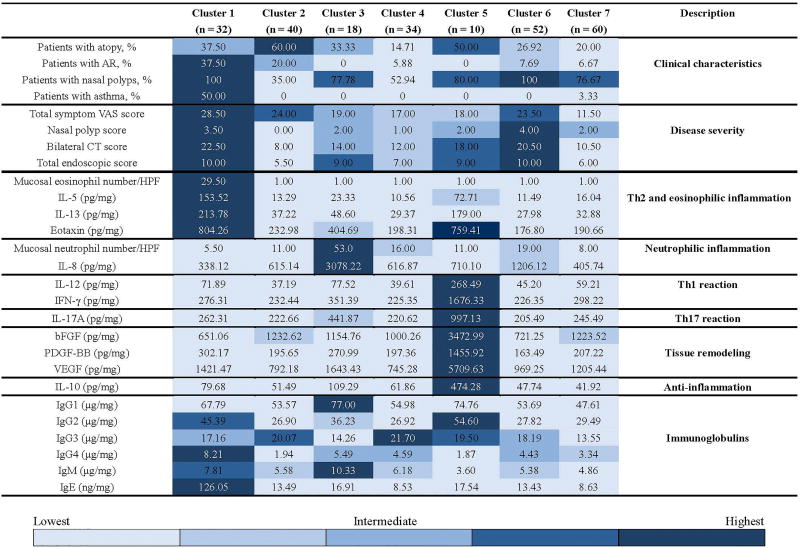
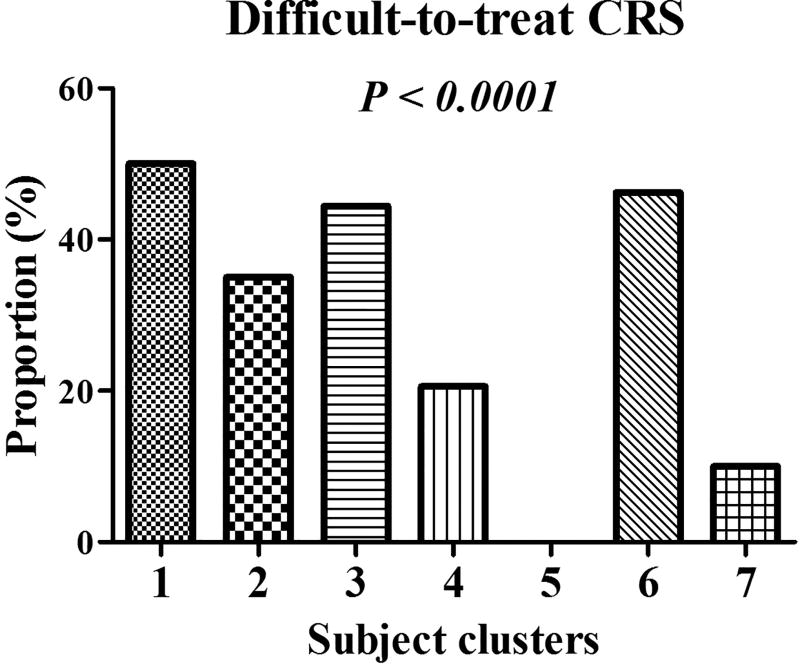
Results: Seven subject clusters were identified. Cluster 1 (13.01%) was comparable to the classic well-defined eosinophilic CRS with polyps, having severe disease and the highest proportion of difficult-to-treat CRS. Patients in cluster 2 (16.26%) and cluster 4 (13.82%) had relatively lower proportions of presence of polyps and presented mild inflammation with moderate proportions of difficult-to-treat cases. Subjects in cluster 2 were highly atopic. Cluster 3 (7.31%) and cluster 6 (21.14%) were characterized by severe or moderate neutrophilic inflammation, respectively, and with elevated levels of IL-8 and high proportions of difficult-to-treat CRS. Cluster 5 (4.07%) was a unique group characterized by the highest levels of IL-10 and lacked difficult-to-treat cases. Cluster 7 (24.39%) demonstrated the lowest symptom severity, a low proportion of difficult-to-treat CRS, and low inflammation load. Finally, we found that difficult-to-treat CRS was associated with distinct clinical features and biomarkers in the different clusters.
Conclusions: Distinct clinicopathobiologic clusters of CRS display differences in clinical response to treatments and characteristics of difficult-to-treat CRS.
Keywords: chronic rhinosinusitis; cluster analysis; difficult-to-treatment; nasal polyps.
© 2018 EAACI and John Wiley and Sons A/S. Published by John Wiley and Sons Ltd.
Conflict of interest statement
Figures
Similar articles
-
Endotypes of chronic rhinosinusitis based on inflammatory and remodeling factors.J Allergy Clin Immunol. 2023 Feb;151(2):458-468. doi: 10.1016/j.jaci.2022.10.010. Epub 2022 Oct 19. J Allergy Clin Immunol. 2023. PMID: 36272582
-
JESREC score and mucosal eosinophilia can predict endotypes of chronic rhinosinusitis with nasal polyps.Auris Nasus Larynx. 2019 Jun;46(3):374-383. doi: 10.1016/j.anl.2018.09.004. Epub 2018 Sep 19. Auris Nasus Larynx. 2019. PMID: 30243753
-
Clinical and cytokine patterns of uncontrolled asthma with and without comorbid chronic rhinosinusitis: a cross-sectional study.Respir Res. 2022 May 11;23(1):119. doi: 10.1186/s12931-022-02028-3. Respir Res. 2022. PMID: 35546400 Free PMC article.
-
Rethinking neutrophils and eosinophils in chronic rhinosinusitis.J Allergy Clin Immunol. 2021 Aug;148(2):327-335. doi: 10.1016/j.jaci.2021.03.024. Epub 2021 Apr 21. J Allergy Clin Immunol. 2021. PMID: 33895002 Free PMC article. Review.
-
A review of current biomarkers in chronic rhinosinusitis with or without nasal polyps.Expert Rev Clin Immunol. 2023 Jul-Dec;19(8):883-892. doi: 10.1080/1744666X.2023.2200164. Epub 2023 Apr 7. Expert Rev Clin Immunol. 2023. PMID: 37017326 Review.
Cited by
-
Recent advances in understanding chronic rhinosinusitis endotypes.F1000Res. 2018 Dec 7;7:F1000 Faculty Rev-1909. doi: 10.12688/f1000research.16222.1. eCollection 2018. F1000Res. 2018. PMID: 30631435 Free PMC article. Review.
-
Budesonide repairs decreased barrier integrity of eosinophilic nasal polyp epithelial cells caused by PM2.5.Clin Transl Allergy. 2021 Jul 3;11(5):e12019. doi: 10.1002/clt2.12029. eCollection 2021 Jul. Clin Transl Allergy. 2021. PMID: 34262692 Free PMC article.
-
Identification of Inflammatory Endotypes by Clinical Characteristics and Nasal Secretion Biomarkers in Chronic Rhinosinusitis with Nasal Polyps.Int Arch Allergy Immunol. 2023;184(10):955-965. doi: 10.1159/000530193. Epub 2023 May 30. Int Arch Allergy Immunol. 2023. PMID: 37253337 Free PMC article.
-
Two-Track Medical Treatment Strategy According to the Clinical Scoring System for Chronic Rhinosinusitis.Allergy Asthma Immunol Res. 2018 Sep;10(5):490-502. doi: 10.4168/aair.2018.10.5.490. Allergy Asthma Immunol Res. 2018. PMID: 30088369 Free PMC article.
-
Prediction of the Active Components and Possible Targets of Xanthii Fructus Based on Network Pharmacology for Use in Chronic Rhinosinusitis.Evid Based Complement Alternat Med. 2022 Feb 3;2022:4473231. doi: 10.1155/2022/4473231. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35287308 Free PMC article.
References
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinology supplement. 2012;23:1–299. - PubMed
-
- Cao PP, Li HB, Wang BF, Wang SB, You XJ, Cui YH, et al. Distinct immunopathologic characteristics of various types of chronic rhinosinusitis in adult Chinese. J Allergy Clin Immunol. 2009;124:478–84. - PubMed
-
- Akdis CA, Bachert C, Cingi C, Dykewicz MS, Hellings PW, Naclerio RM, et al. Endotypes and phenotypes of chronic rhinosinusitis A PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2013;131:1479–90. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
