

Overall survival and oncological outcomes after partial nephrectomy and radical nephrectomy for cT2a renal tumors: A collaborative international study from the French kidney cancer research network UroCCR
- PMID: 29331568
- PMCID: PMC9084631
- DOI: 10.1016/j.purol.2017.12.004
Overall survival and oncological outcomes after partial nephrectomy and radical nephrectomy for cT2a renal tumors: A collaborative international study from the French kidney cancer research network UroCCR
Abstract
Background: Partial nephrectomy (PN) is recommended as first-line treatment for cT1 stage kidney tumors because of a better renal function and probably a better overall survival than radical nephrectomy (RN). For larger tumors, PN has a controversial position due to lack of evidence showing good cancer control. The aim of this study was to compare the results of PN and RN in cT2a stage on overall survival and oncological results.
Method: A retrospective international multicenter study was conducted in the frame of the French kidney cancer research network (UroCCR). We considered all patients aged≥18 years who underwent surgical treatment for localized renal cell carcinoma (RCC) stage cT2a (7.1-10cm) between 2000 and 2014. Cox and Fine-Gray models were performed to analyze overall survival (OS), cancer specific survival (CSS) and cancer-free survival (CFS). Comparison between PN and RN was realized after an adjustment by propensity score considering predefined confounding factors: age, sex, tumor size, pT stage of the TNM classification, histological type, ISUP grade, ASA score.
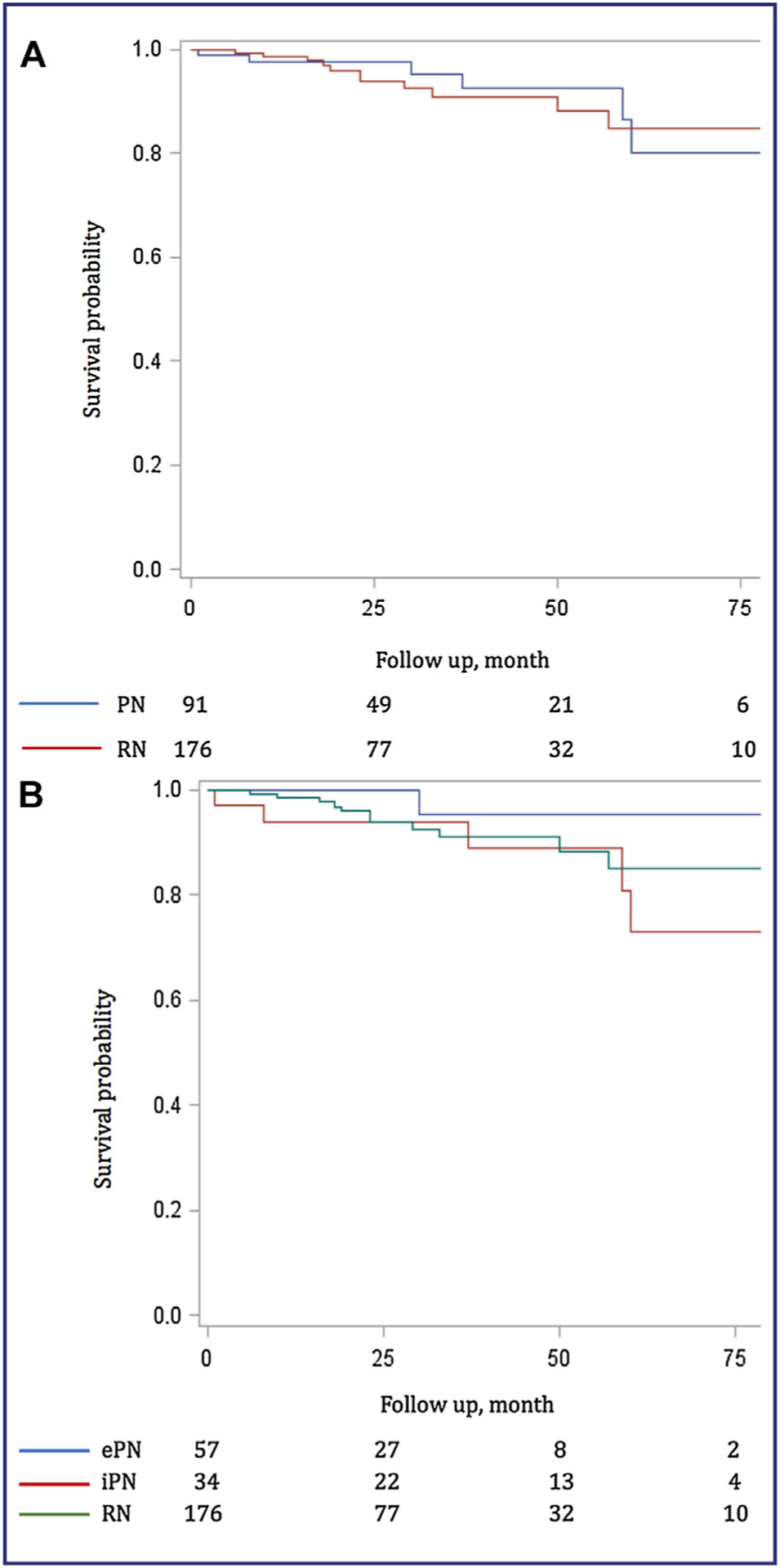
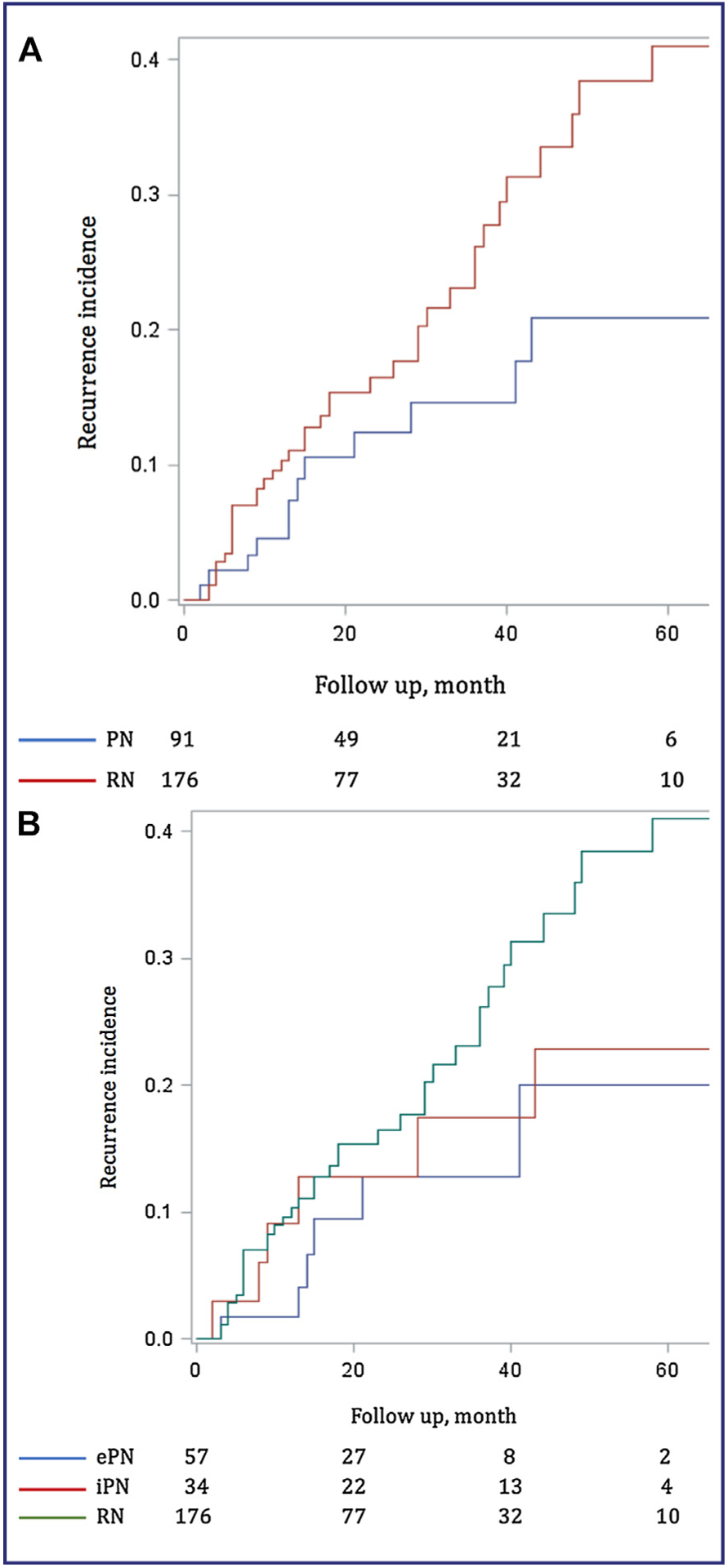
Results: A total of 267 patients were included. OS at 3 and 5 years was 93.6% and 78.7% after PN and 88.0% and 76.2% after RN, respectively. CSS at 3 and 5 years was 95.4% and 80.2% after PN and 91.0% and 85.0% after RN. No significant difference between groups was found after propensity score adjustment for OS (HR 0.87, 95% CI: 0.37-2.05, P=0.75), CSS (HR 0.52, 95% CI: 0.18-1.54, P=0.24) and CFS (HR 1.02, 95% CI: 0.50-2.09, P=0.96).
Conclusion: PN seems equivalent to RN for OS, CSS and CFS in cT2a stage kidney tumors. The risk of recurrence is probably more related to prognostic factors than the surgical technique. The decision to perform a PN should depend on technical feasibility rather than tumor size, both to imperative and elective situation.
Level of evidence: 4.
Contexte. –: La néphrectomie partielle (NP) est recommandée en première intention pour les tumeurs du rein de stades cT1. Sa place est débattue pour les stades cT2 en raison du manque de preuve d’un bon contrôle carcinologique. L’objectif de cette étude était de comparer les résultats de la NP et de la néphrectomie élargie (NE) dans les stades cT2a sur la survie globale et les résultats oncologiques.
Méthode. –: Une étude rétrospective multicentrique internationale était menée à partir de bases de données de 15 centres. Tous les patients d’âge ≥ 18 ans ayant bénéficié d’un traitement chirurgical pour un CCR localisé de stade cT2a (7,1–10 cm) entre 2000 et 2014 étaient inclus. La comparaison entre NP et NE était effectuée après ajustement par score ASA et par score de propension tenant compte des facteurs de confusion prédéfinis : âge, sexe, taille tumorale, stade pT de la classification TNM, type histologique, grade ISUP.
Résultats. –: Au total, 267 patients étaient inclus. La survie globale (SG) à 3 et 5 ans était de 93,6 % et 78,7 % dans le groupe NP et de 88,0 % et 76,2 % dans le groupe NE. La survie spécifique (SSp) à 3 et 5 ans était de 95,4 % et 80,2 % dans le groupe NP et de 91,0 % et 85,0 % dans le groupe NE. Aucune différence significative entre les deux groupes n’était retrouvée après ajustement sur le score de propension pour la SG (HR 0,87, IC 0,37–2,05, p = 0,75), la SSp (HR 0,52, IC 0,18–1,54, p = 0,24) et la Survie sans récidive (SSR) (HR 1,02, IC 0,50–2,09, p = 0,96).
Conclusion. –: Les résultats de la NP semblent équivalents à la NE pour la SG, la SSp et la SSR. Le risque de récidive semble davantage lié aux facteurs pronostiques qu’à la technique chirurgicale. La décision de NP devrait dépendre de sa faisabilité technique plutôt que de la taille tumorale, aussi bien en situation élective qu’impérative.
Niveau de preuve.–: 4.
Keywords: Cancer du rein; Néphrectomie partielle; Oncology; Outcomes; Partial nephrectomy; Renal cancer; Résultats oncologiques; Sparing surgery; Survie globale.
Copyright © 2017 Elsevier Masson SAS. All rights reserved.
Conflict of interest statement
Disclosure of interest
The authors have not supplied their declaration of competing interest.
Figures

Similar articles
-
Oncological outcomes of minimally invasive partial versus minimally invasive radical nephrectomy for cT1-2/N0/M0 clear cell renal cell carcinoma: a propensity score-matched analysis.World J Urol. 2017 May;35(5):789-794. doi: 10.1007/s00345-016-1923-2. Epub 2016 Aug 30. World J Urol. 2017. PMID: 27578234
-
[A retrospective matching study of partial nephrectomy and radical nephrectomy for pathological T3a stage renal cell carcinoma].Beijing Da Xue Xue Bao Yi Xue Ban. 2025 Aug 18;57(4):704-710. doi: 10.19723/j.issn.1671-167X.2025.04.012. Beijing Da Xue Xue Bao Yi Xue Ban. 2025. PMID: 40754907 Chinese.
-
Survival after partial and radical nephrectomy for the treatment of stage T1bN0M0 renal cell carcinoma (RCC) in the USA: a propensity scoring approach.BJU Int. 2012 May;109(10):1457-62. doi: 10.1111/j.1464-410X.2011.10597.x. Epub 2011 Sep 20. BJU Int. 2012. PMID: 21933334
-
Comparison of the long-term follow-up and perioperative outcomes of partial nephrectomy and radical nephrectomy for 4 cm to 7 cm renal cell carcinoma: a systematic review and meta-analysis.BMC Urol. 2019 Jun 7;19(1):48. doi: 10.1186/s12894-019-0480-6. BMC Urol. 2019. PMID: 31174522 Free PMC article.
-
Partial nephrectomy versus radical nephrectomy for large (≥ 7 cm) renal tumors: A systematic review and meta-analysis.Urol Oncol. 2019 Apr;37(4):263-272. doi: 10.1016/j.urolonc.2018.12.015. Epub 2019 Jan 28. Urol Oncol. 2019. PMID: 30704957
Cited by
-
Surgical Experience and Functional Outcomes after Laparoscopic and Robot-Assisted Partial Nephrectomy: Results from a Multi-Institutional Collaboration.J Clin Med. 2024 Oct 9;13(19):6016. doi: 10.3390/jcm13196016. J Clin Med. 2024. PMID: 39408076 Free PMC article.
-
Partial Nephrectomy Versus Radical Nephrectomy for Clinical T2 or Higher Stage Renal Tumors: A Systematic Review and Meta-Analysis.Front Oncol. 2021 Jun 10;11:680842. doi: 10.3389/fonc.2021.680842. eCollection 2021. Front Oncol. 2021. PMID: 34178668 Free PMC article.
-
Artificial Intelligence-Based Prognostic Model for Urologic Cancers: A SEER-Based Study.Cancers (Basel). 2022 Jun 26;14(13):3135. doi: 10.3390/cancers14133135. Cancers (Basel). 2022. PMID: 35804904 Free PMC article.
-
Efficacy and safety of surgery in renal carcinoma patients 75 years and older: a retrospective analysis.BMC Urol. 2022 Aug 29;22(1):135. doi: 10.1186/s12894-022-01088-3. BMC Urol. 2022. PMID: 36038864 Free PMC article.
-
Selective Arterial Embolization of Pseudoaneurysms and Arteriovenous Fistulas after Partial Nephrectomy: Safety, Efficacy, and Mid-Term Outcomes.Biomedicines. 2023 Jul 7;11(7):1935. doi: 10.3390/biomedicines11071935. Biomedicines. 2023. PMID: 37509574 Free PMC article.
References
-
- Chow WH, Devesa SS, Warren JL, Fraumeni JF. Rising incidence of renal cell cancer in the United States. JAMA 1999;281(17):1628–31. - PubMed
-
- Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst 2006;98(18):1331–4. - PubMed
-
- Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Five-year survival after surgical treatment for kidney cancer: a population-based competing risk analysis. Cancer 2007;109(9):1763–8. - PubMed
-
- Astor BC, Hallan SI, Miller ER, Yeung E, Coresh J. Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the US population. Am J Epidemiol 2008;167(10):1226–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
