

Probenecid Improves Cardiac Function in Patients With Heart Failure With Reduced Ejection Fraction In Vivo and Cardiomyocyte Calcium Sensitivity In Vitro
- PMID: 29331959
- PMCID: PMC5850150
- DOI: 10.1161/JAHA.117.007148
Probenecid Improves Cardiac Function in Patients With Heart Failure With Reduced Ejection Fraction In Vivo and Cardiomyocyte Calcium Sensitivity In Vitro
Abstract
Background: Transient receptor potential vanilloid 2 is a calcium channel activated by probenecid. Probenecid is a Food and Drug Administration-approved uricosuric drug that has recently been shown to induce positive lusitropic and inotropic effects in animal models through cardiomyocyte transient receptor potential vanilloid 2 activation. The aim of this study was to test the hypothesis that oral probenecid can improve cardiac function and symptomatology in patients with heart failure with reduced ejection fraction and to further elucidate its calcium-dependent effects on myocyte contractility.
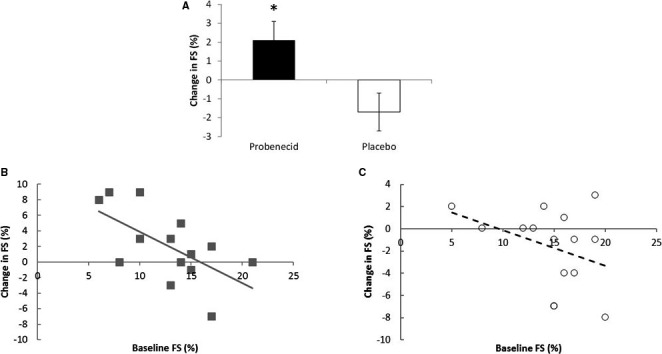
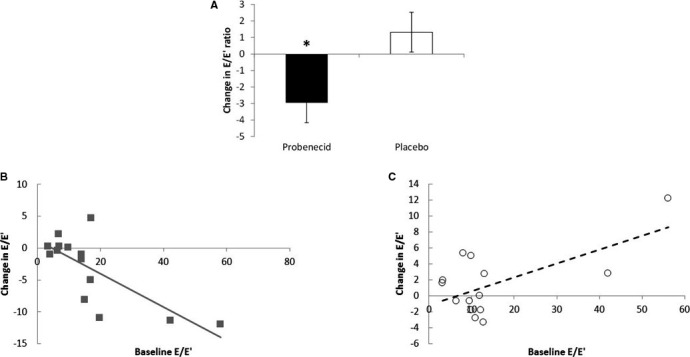
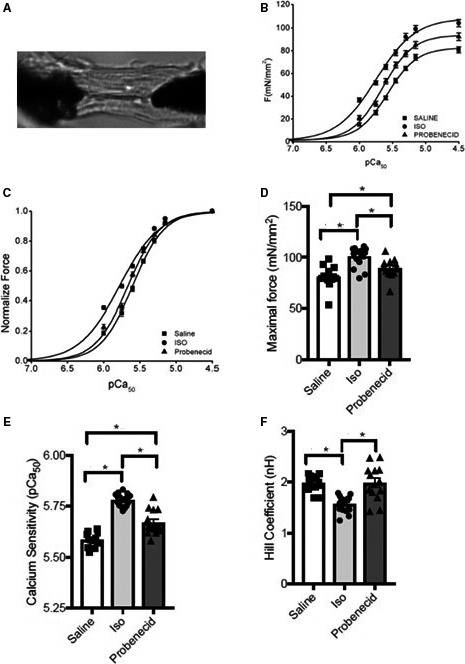
Methods and results: The clinical trial recruited stable outpatients with heart failure with reduced ejection fraction randomized in a single-center, double-blind, crossover design. Clinical data were collected including a dyspnea assessment, physical examination, ECG, echocardiogram to assess systolic and diastolic function, a 6-minute walk test, and laboratory studies. In vitro force generation studies were performed on cardiomyocytes isolated from murine tissue exposed to probenecid or control treatments. The clinical trial recruited 20 subjects (mean age 57 years, mean baseline fractional shortening of 13.6±1.0%). Probenecid therapy increased fractional shortening by 2.1±1.0% compared with placebo -1.7±1.0% (P=0.007). Additionally, probenecid improved diastolic function compared with placebo by decreasing the E/E' by -2.95±1.21 versus 1.32±1.21 in comparison to placebo (P=0.03). In vitro probenecid increased myofilament force generation (92.36 versus 80.82 mN/mm2, P<0.05) and calcium sensitivity (pCa 5.67 versus 5.60, P<0.01) compared with control.
Conclusions: Probenecid improves cardiac function with minimal effects on symptomatology and no significant adverse effects after 1 week in patients with heart failure with reduced ejection fraction and increases force development and calcium sensitivity at the cardiomyocyte level.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT01814319.
Keywords: Probenecid; TRPV2; echocardiography.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Gheorghiade M, Zannad F, Sopko G, Klein L, Piña IL, Konstam MA, Massie BM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L. Acute heart failure syndromes: current state and framework for future research. Circulation. 2005;112:3958–3968. - PubMed
-
- Abraham WT, Adams KF, Fonarow GC, Costanzo MR, Berkowitz RL, LeJemtel TH, Cheng ML, Wynne J. In‐hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am Coll Cardiol. 2005;46:57–64. - PubMed
-
- Endoh M. Ca 2+ in cardiac E‐C coupling. Circ J. 2008;72:1915–1925. Available at: https://www.jstage.jst.go.jp/article/circj/72/12/72_CJ-08-0838/_pdf. Accessed June 28, 2017. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
