

Temporal trends in antithrombotic treatment of real-world UK patients with newly diagnosed atrial fibrillation: findings from the GARFIELD-AF registry
- PMID: 29331969
- PMCID: PMC5781154
- DOI: 10.1136/bmjopen-2017-018905
Temporal trends in antithrombotic treatment of real-world UK patients with newly diagnosed atrial fibrillation: findings from the GARFIELD-AF registry
Abstract
Objective: To investigate evolving patterns in antithrombotic treatment in UK patients with newly diagnosed non-valvular atrial fibrillation (AF).
Design: Prospective, multicentre, international registry.
Setting: 186 primary care practices in the UK.
Participants: 3482 participants prospectively enrolled in four sequential cohorts (cohort 2 (C2) n=830, diagnosed September 2011 to April 2013; cohort 3 (C3) n=902, diagnosed April 2013 to June 2014; cohort 4 (C4) n=850, diagnosed July 2014 to June 2015; cohort 5 (C5) n=900, diagnosed June 2015 to July 2016). Participants had newly diagnosed non-valvular AF and at least one risk factor for stroke, were aged ≥18, and provided informed consent.
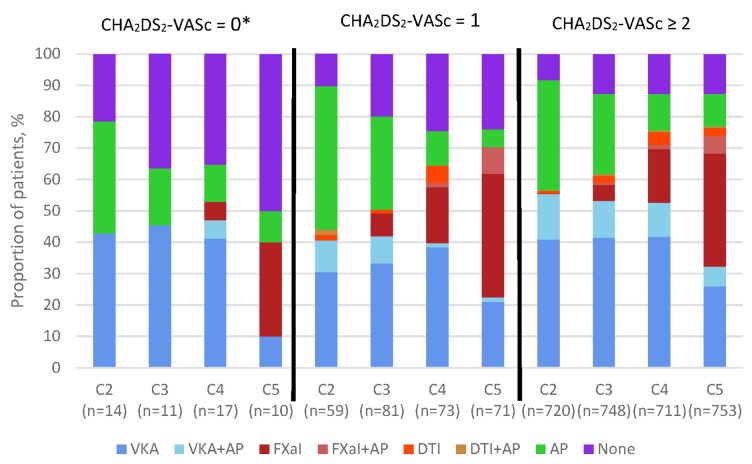
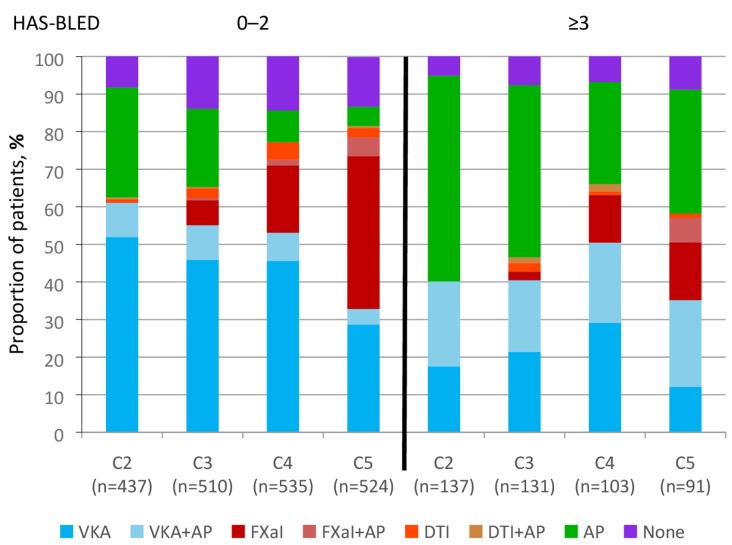
Main outcome measures: Antithrombotic treatment initiated at diagnosis, overall and according to stroke and bleeding risks. Stroke risk was retrospectively calculated using CHA2DS2-VASc (cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled)-vascular disease, age 65-74 and sex category (female)) and bleeding risk using HAS-BLED (hypertension, abnormal renal/liver function (1 point each), stroke, bleeding history or predisposition, elderly (>65), drugs/alcohol concomitantly (1 point each)).
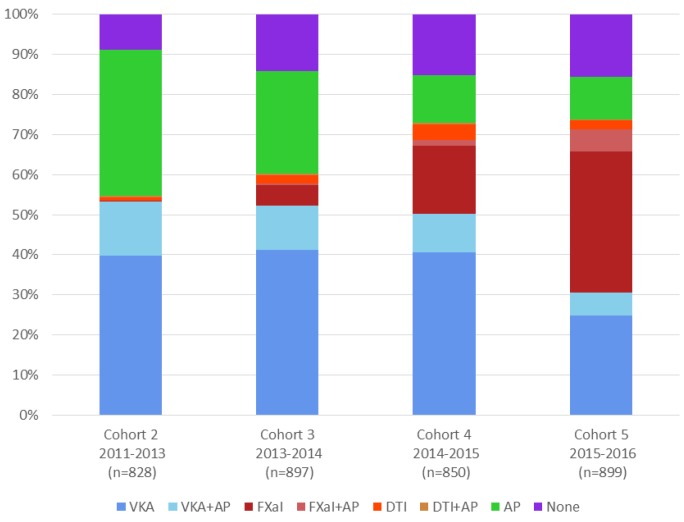
Results: 42.7% were women and the mean age was 74.5 years. The median CHA2DS2-VASc score was 3 in all cohorts and the median HAS-BLED score was 2 in all cohorts. There was a statistically significant increase in the use of anticoagulant therapy from C2 to C5 (C2 54.7%, C3 60.3%, C4 73.1%, C5 73.9%; P value for trend <0.0001). The increase in the use of anticoagulant was mainly in patients with CHA2DS2-VASc ≥2. The use of vitamin K antagonists (VKAs)±antiplatelet (AP) drugs decreased from C2 to C5 (C2 53.3%, C3 52.1%, C4 50.3%, C5 30.6%), while the use of non-vitamin K antagonist oral anticoagulants (NOACs)±AP increased (C2 1.3%, C3 8.0%, C4 22.7%, C5 43.3%). The use of AP only decreased (C2 36.4%, C3 25.5%, C4 11.9%, C5 10.5%), as did the combination therapy of VKA+AP (C2 13.6%, C3 11.0%, C4 9.6%, C5 5.8%).
Conclusion: There has been a progressive increase in the proportion of patients newly diagnosed with AF receiving guideline-recommended therapy in the UK, potentially driven by the availability of NOACs.
Trial registration number: NCT01090362; Pre-results.
Keywords: anticoagulation; antithrombotic therapy; atrial fibrillation; newly diagnosed; stroke prophylaxis.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: FDRH personal fees and other from BMS/Pfizer, personal fees and other from BI, personal fees and other from Bayer, outside the submitted work.
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med 1987;147:1561–4. - PubMed
-
- National Instisute for Health and Clinical Excellence (NICE). Nice Clinical Guideline 180; Atrial Fibrillation: the management of atrial fibrillation. 2014. https://www.nice.org.uk/guidance/cg180
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous