

Robot-Assisted Radical Prostatectomy Is More Beneficial for Prostate Cancer Patients: A System Review and Meta-Analysis
- PMID: 29332100
- PMCID: PMC5776881
- DOI: 10.12659/msm.907092
Robot-Assisted Radical Prostatectomy Is More Beneficial for Prostate Cancer Patients: A System Review and Meta-Analysis
Abstract
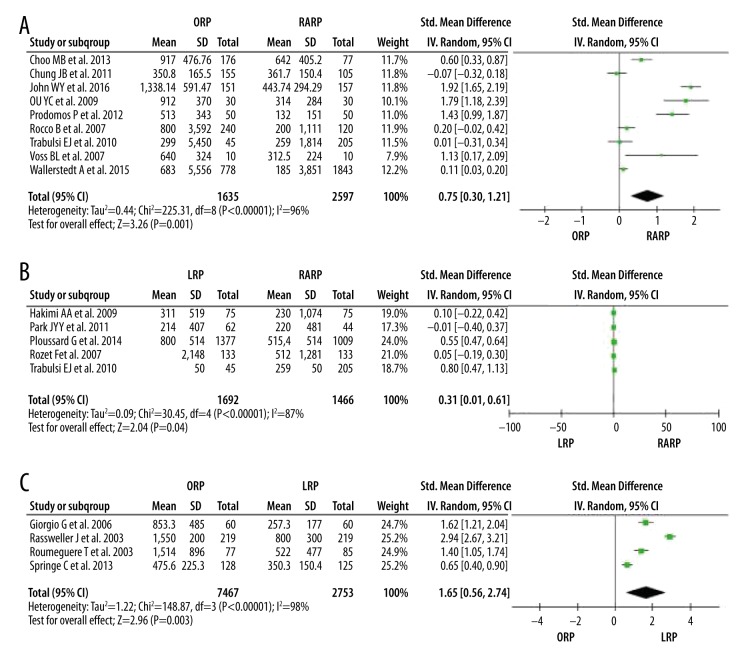
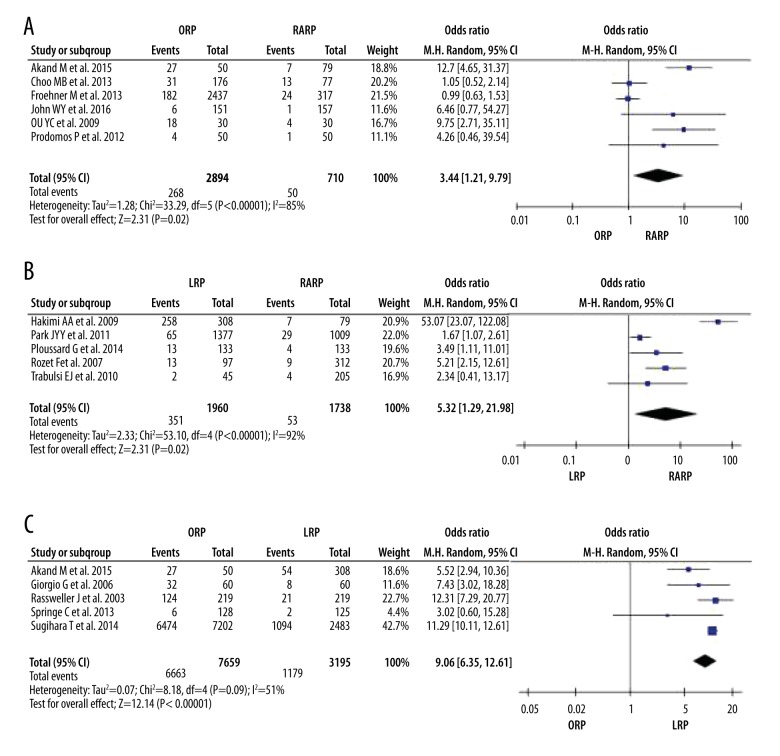
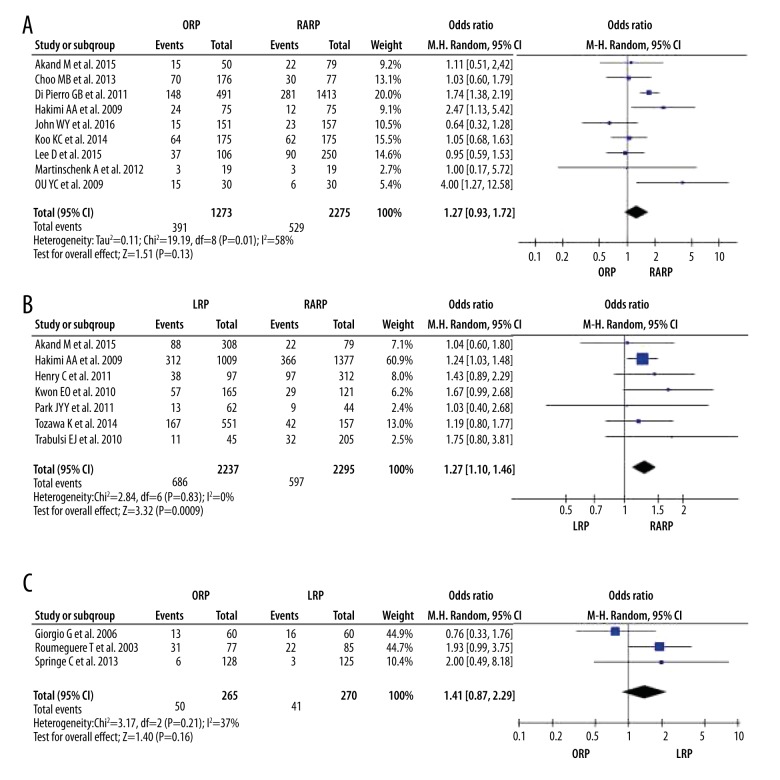
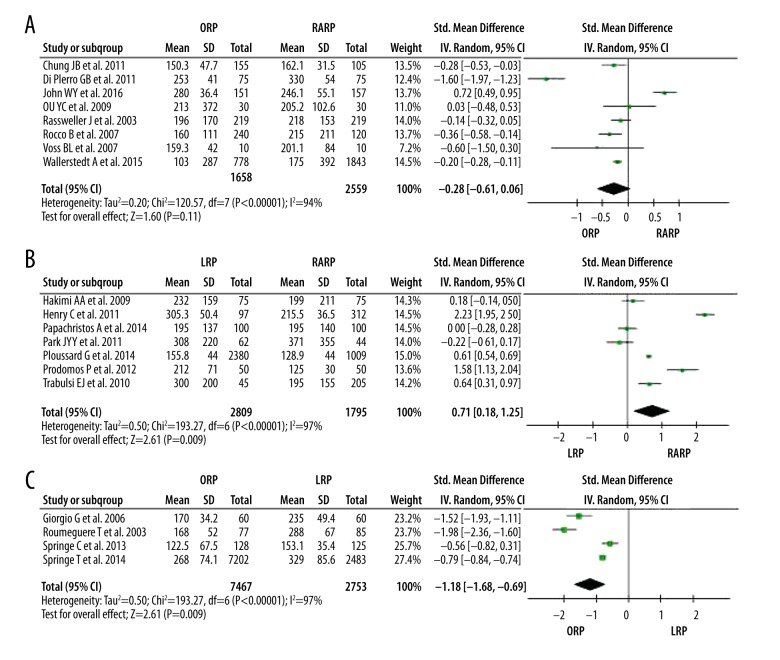
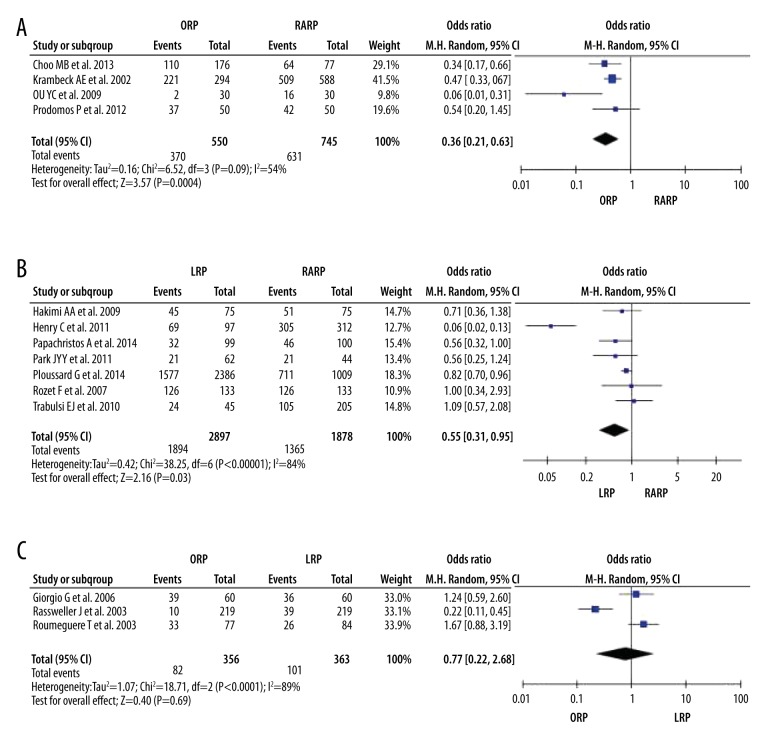
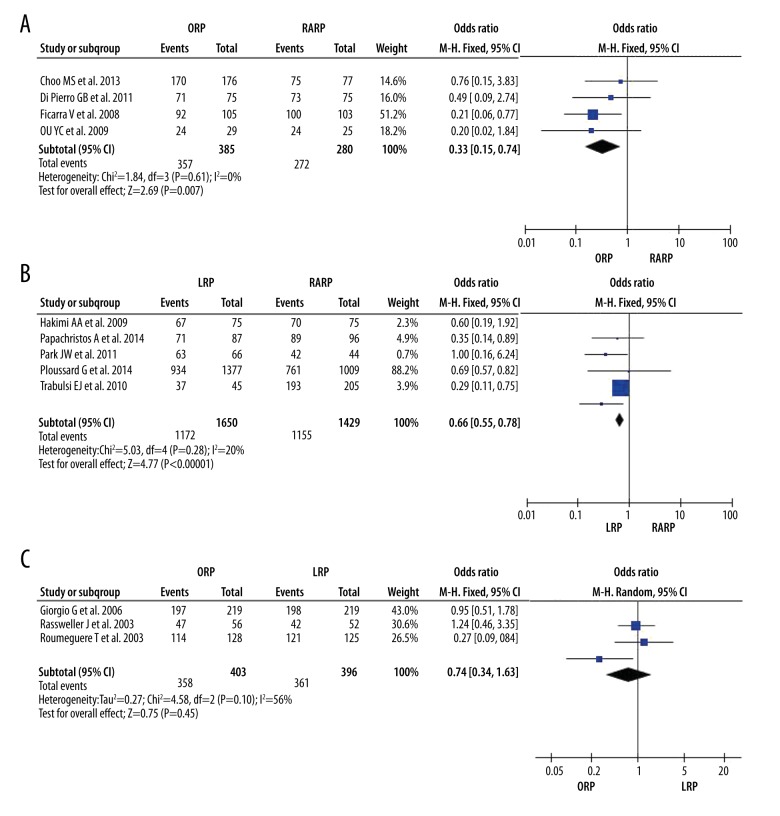
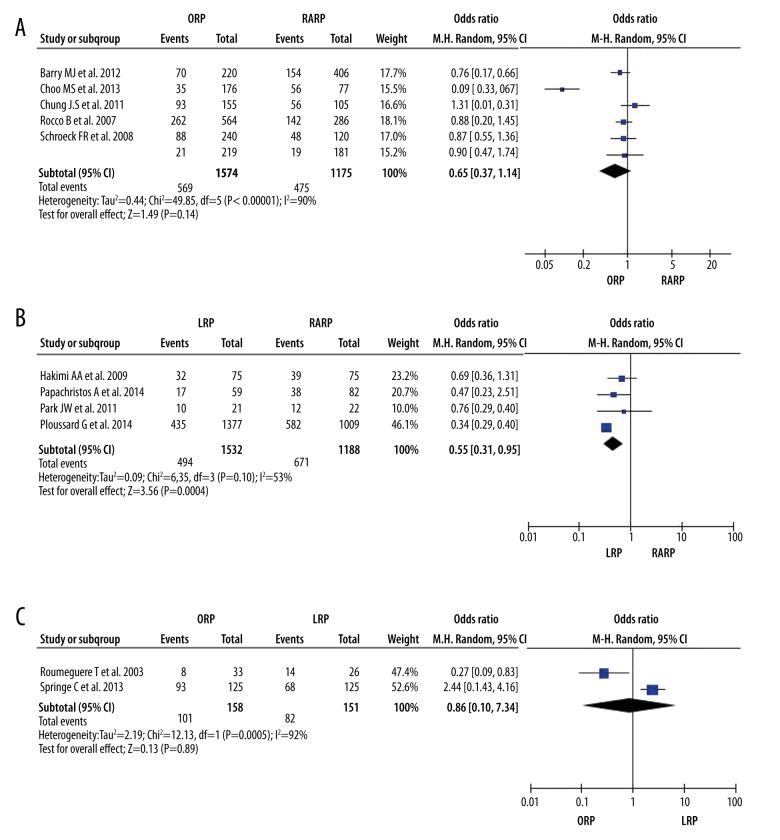
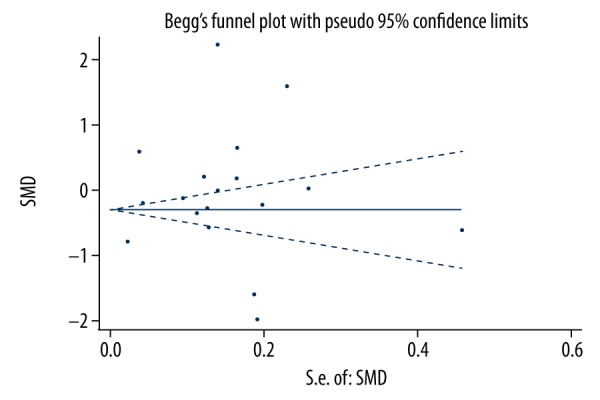
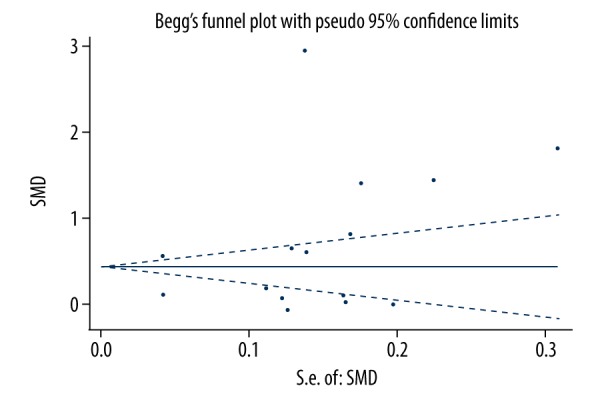
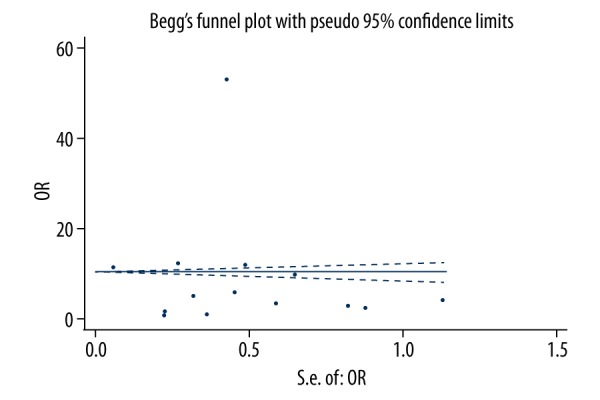
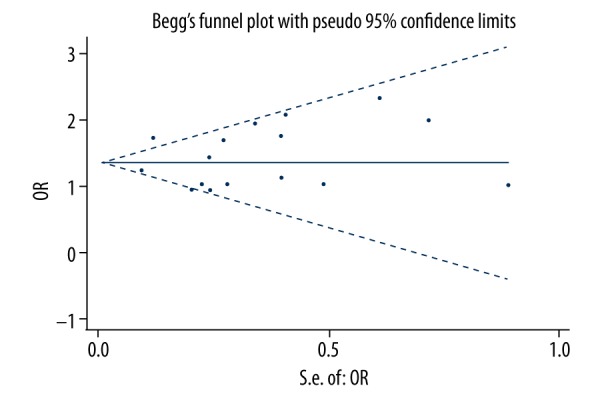
BACKGROUND Robot-assisted radical prostatectomy (RARP) is increasingly used worldwide, but comparisons of perioperative, functional, and oncologic outcomes among RARP, laparoscopic radical prostatectomy (LRP), and open radical prostatectomy (ORP) remain inconsistent. MATERIAL AND METHODS Systematic literature searches were conducted using EMBASE, PubMed, the Cochrane Library, CNKI, and Science Direct/Elsevier up to April 2017. A meta-analysis was conducted using Review Manager and Stata software. RESULTS We included 33 studies. Meta-analysis revealed that blood loss, transfusion rate, and positive surgical margin (PSM) rate were significantly lower following RARP compared with LRP (SMD (95% confidence interval [CI]) 0.31 [0.01, 0.61]; combined ORs (95% CI) 5.32 [1.29, 21.98]; 1.27 [1.10, 1.46]) and ORP (SMD (95% CI) 0.75 [0.30, 1.21]; and combined ORs (95% CI) 3.44 [1.21, 9.79]); positive surgical margin (PSM) rates were significantly lower following RARP compared with LRP (combined ORs (95% CI) 1.27 [1.10, 1.46]), but not ORP. Operation time was also shorter for RARP than for LRP. The rates of nerve-sparing, recovery of complete urinary continence, and recovery of erectile function were significantly higher following RARP compared with LRP (combined ORs (95% CI) 0.55 [0.31, 0.95]; 0.66 [0.55, 0.78]; 0.46 [0.30, 0.71]) and ORP (combined ORs (95% CI) 0.36 [0.21, 0.63]; 0.33 [0.15, 0.74]; 0.65 [0.37, 1.14]). CONCLUSIONS This meta-analysis demonstrates that RARP results in better overall outcomes than LRP and ORP in terms of blood loss, transfusion rate, nerve sparing, urinary continence and erectile dysfunction recovery, and suggests that RARP offers better results than LRP and ORP in treatment of prostate cancer. However, studies with larger sample sizes and long-term results are needed.
Conflict of interest statement
None.
Figures
References
-
- Raboy A, Ferzli G, Albert P. Initial experience with extraperitoneal endoscopic radical retropubic prostatectomy. Urology. 1997;50:849–53. - PubMed
-
- Rassweiler J, Seemann O, Schulze M, et al. Laparoscopic versus open radical prostatectomy: A comparative study at a single institution. J Urol. 2003;169:1689–93. - PubMed
-
- Anastasiadis AG, Salomon L, Katz R, et al. Radical retropubic versus laparoscopic prostatectomy: A prospective comparison of functional outcome. Urology. 2003;62:292–97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
