

Tricuspid flow and regurgitation in congenital heart disease and pulmonary hypertension: comparison of 4D flow cardiovascular magnetic resonance and echocardiography
- PMID: 29332606
- PMCID: PMC5767973
- DOI: 10.1186/s12968-017-0426-7
Tricuspid flow and regurgitation in congenital heart disease and pulmonary hypertension: comparison of 4D flow cardiovascular magnetic resonance and echocardiography
Abstract
Background: Tricuspid valve (TV) regurgitation (TR) is a common complication of pulmonary hypertension and right-sided congenital heart disease, associated with increased morbidity and mortality. Estimation of TR severity by echocardiography and conventional cardiovasvular magnetic resonance (CMR) is not well validated and has high variability. 4D velocity-encoded (4D-flow) CMR was used to measure tricuspid flow in patients with complex right ventricular (RV) geometry and varying degrees of TR. The aims of the present study were: 1) to assess accuracy of 4D-flow CMR across the TV by comparing 4D-flow CMR derived TV effective flow to 2D-flow derived effective flow across the pulmonary valve (PV); 2) to assess TV 4D-flow CMR reproducibility, and 3) to compare TR grade by 4D-flow CMR to TR grade by echocardiography.
Methods: TR was assessed by both 4D-flow CMR and echocardiography in 21 healthy subjects (41.2 ± 10.5 yrs., female 7 (33%)) and 67 RV pressure-load patients (42.7 ± 17.0 yrs., female 32 (48%)). The CMR protocol included 4D-flow CMR measurement across the TV, 2D-flow measurement across the PV and conventional planimetric measurements. TR grading on echocardiographic images was performed based on the international recommendations. Bland-Altman analysis and intra-class correlation coefficients (ICC) were used to asses correlations and agreement.
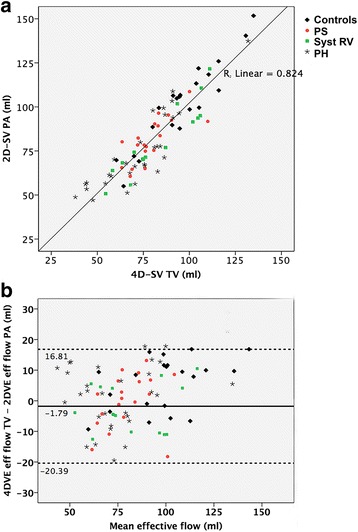
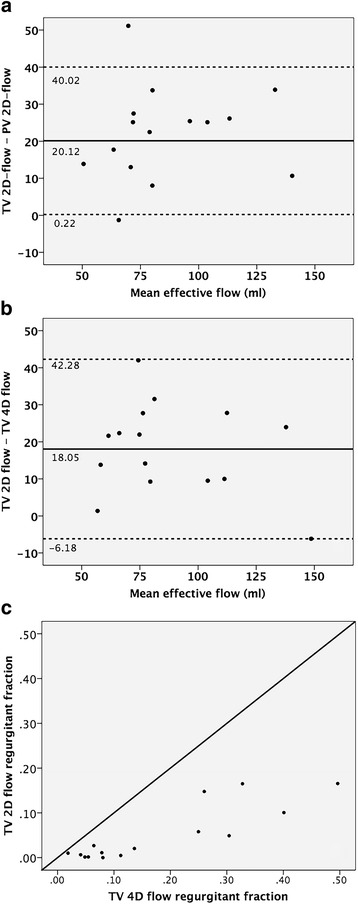
Results: TV effective flow measured by 4D-flow CMR showed good correlation and agreement with PV effective flow measured by 2D-flow CMR with ICC = 0.899 (p < 0.001) and mean difference of -1.79 ml [limits of agreement -20.39 to 16.81] (p = 0.084). Intra-observer agreement for effective flow (ICC = 0.981; mean difference - 1.51 ml [-12.88 to 9.86]) and regurgitant fraction (ICC = 0.910; mean difference 1.08% [-7.90; 10.06]) was good. Inter-observer agreement for effective flow (ICC = 0.935; mean difference 2.12 ml [-15.24 to 19.48]) and regurgitant fraction (ICC = 0.968; mean difference 1.10% [-7.96 to 5.76]) were comparable. In 25/65 (38.5%) TR grade differed by at least 1 grade using 4D-flow CMR compared to echocardiography.
Conclusion: TV effective flow derived from 4D-flow CMR showed excellent correlation to PV effective flow derived from 2D-flow CMR, and was reproducible to measure TV flow and regurgitation. Twenty-five out of 65 patients (38.5%) were classified differently by at least one TR grade using 4D-flow CMR compared to echocardiography.
Keywords: 4D-flow MRI; Congenital heart disease; Echocardiography; Pulmonary hypertension; Tricuspid regurgitation.
Conflict of interest statement
Authors’ information
Not applicable.
Dr. John Oshinski served as a Guest Editor for this manuscript.
Ethics approval and consent to participate
The Ethical Review boards of all participating centers approved the study and written informed consent was obtained from all participants prior to inclusion. The primary ethical review committee was at University medical Center Utrecht (number METC-11-003). The ethical review boards of both Radboud University medical Center (number 2011/329) and Antonius Hospital Nieuwegein (number LTME/L-11.34/RV-def) also extended their approval.
Consent for publication
In the current manuscript, data is not reducible to a patient. However, in all patients consent for publication was obtained in all patients upon prior to inclusion (part of informed consent).
Competing interests
The authors declare that they have no competing interests. M.P. has received lecture fees from Bayer, Actelion and Pfizer. M.D. has received a research grant from the ICIN-Netherlands heart house (Utrecht, the Netherlands).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
Direct measurement of atrioventricular valve regurgitant jets using 4D flow cardiovascular magnetic resonance is accurate and reliable for children with congenital heart disease: a retrospective cohort study.J Cardiovasc Magn Reson. 2020 May 14;22(1):33. doi: 10.1186/s12968-020-00612-4. J Cardiovasc Magn Reson. 2020. PMID: 32404159 Free PMC article.
-
Validation of aortic valve 4D flow analysis and myocardial deformation by cardiovascular magnetic resonance in patients after the arterial switch operation.J Cardiovasc Magn Reson. 2019 Mar 18;21(1):20. doi: 10.1186/s12968-019-0527-6. J Cardiovasc Magn Reson. 2019. PMID: 30879465 Free PMC article.
-
3D Echocardiographic and CMR Imaging for the Assessment of Right Ventricular Function and Tricuspid Regurgitation Severity.Circ Cardiovasc Imaging. 2025 Apr;18(4):e017638. doi: 10.1161/CIRCIMAGING.124.017638. Epub 2025 Mar 21. Circ Cardiovasc Imaging. 2025. PMID: 40116010
-
3-Dimensional Echocardiography in Imaging the Tricuspid Valve.JACC Cardiovasc Imaging. 2019 Mar;12(3):500-515. doi: 10.1016/j.jcmg.2018.10.035. JACC Cardiovasc Imaging. 2019. PMID: 30846124 Review.
-
All you need to know about the tricuspid valve: Tricuspid valve imaging and tricuspid regurgitation analysis.Arch Cardiovasc Dis. 2016 Jan;109(1):67-80. doi: 10.1016/j.acvd.2015.08.007. Epub 2015 Dec 23. Arch Cardiovasc Dis. 2016. PMID: 26711544 Review.
Cited by
-
4D Flow MRI Quantification of Congenital Shunts: Comparison to Invasive Catheterization.Radiol Cardiothorac Imaging. 2021 Apr 1;3(2):e200446. doi: 10.1148/ryct.2021200446. eCollection 2021 Apr. Radiol Cardiothorac Imaging. 2021. PMID: 33969306 Free PMC article.
-
Assessment of Tricuspid Regurgitation by Cardiac Magnetic Resonance Imaging: Current Role and Future Applications.J Clin Med. 2024 Jul 31;13(15):4481. doi: 10.3390/jcm13154481. J Clin Med. 2024. PMID: 39124748 Free PMC article. Review.
-
Tricuspid valve flow measurement using a deep learning framework for automated valve-tracking 2D phase contrast.Magn Reson Med. 2024 Nov;92(5):1838-1850. doi: 10.1002/mrm.30163. Epub 2024 May 31. Magn Reson Med. 2024. PMID: 38817154
-
Diastolic dysfunction evaluation by cardiovascular magnetic resonance derived E, a, e': Comparison to echocardiography.Physiol Rep. 2024 Dec;12(23):e70078. doi: 10.14814/phy2.70078. Physiol Rep. 2024. PMID: 39604208 Free PMC article.
-
Non-enhanced MRI flow evaluation using 4D versus 2D phase-contrast in repaired Tetralogy of Fallot adults.Eur Radiol. 2025 Apr 17. doi: 10.1007/s00330-025-11542-z. Online ahead of print. Eur Radiol. 2025. PMID: 40244407
References
-
- Dandel M, Knosalla C, Kemper D, Stein J, Hetzer R. Assessment of right ventricular adaptability to loading conditions can improve the timing of listing to transplantation in patients with pulmonary arterial hypertension. J Heart Lung Transplant. 2015;34:319–328. doi: 10.1016/j.healun.2014.11.012. - DOI - PubMed
-
- Valente AM, Cook S, Festa P, Ko HH, Krishnamurthy R, Taylor AM, et al. Multimodality imaging guidelines for patients with repaired tetralogy of fallot: a report from the AmericanSsociety of echocardiography: developed in collaboration with the Society for Cardiovascular Magnetic Resonance and the Society for Pediatric Radiology. J Am Soc Echocardiogr. 2014;27:111–141. doi: 10.1016/j.echo.2013.11.009. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
