

Induction Chemotherapy in Technically Unresectable Locally Advanced T4a Oral Cavity Squamous Cell Cancers: Experience from a Regional Cancer Center of South India
- PMID: 29333018
- PMCID: PMC5759070
- DOI: 10.4103/ijmpo.ijmpo_185_16
Induction Chemotherapy in Technically Unresectable Locally Advanced T4a Oral Cavity Squamous Cell Cancers: Experience from a Regional Cancer Center of South India
Abstract
Objectives: The present study aimed to investigate the efficacy, toxicity, and impact of induction chemotherapy (IC) in technically unresectable T4a oral cavity squamous cell cancers (OSCCs).
Materials and methods: Patients diagnosed with technically unresectable locally advanced T4a OSCC from January 2013 and November 2016 at our center, who received 2-3 cycles of IC and then assessed for resectability, were reviewed retrospectively. Patients' profile, response rates and toxicity of IC, resectability status, and overall survival (OS) were evaluated. Statistical analyses were performed using SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL, USA).
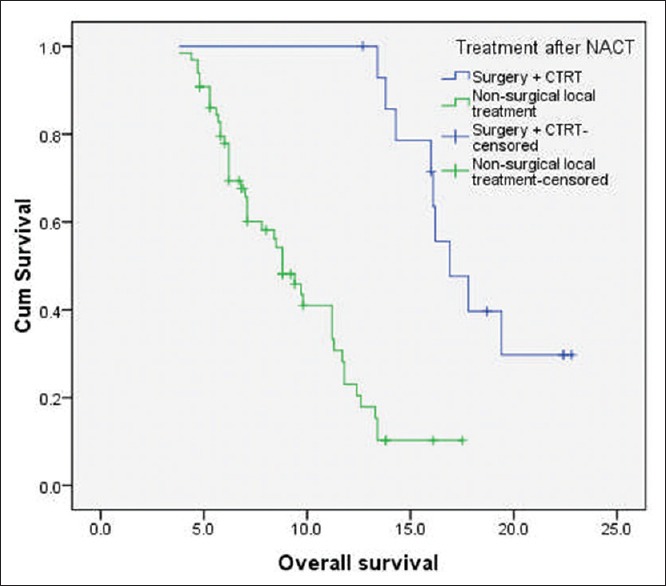
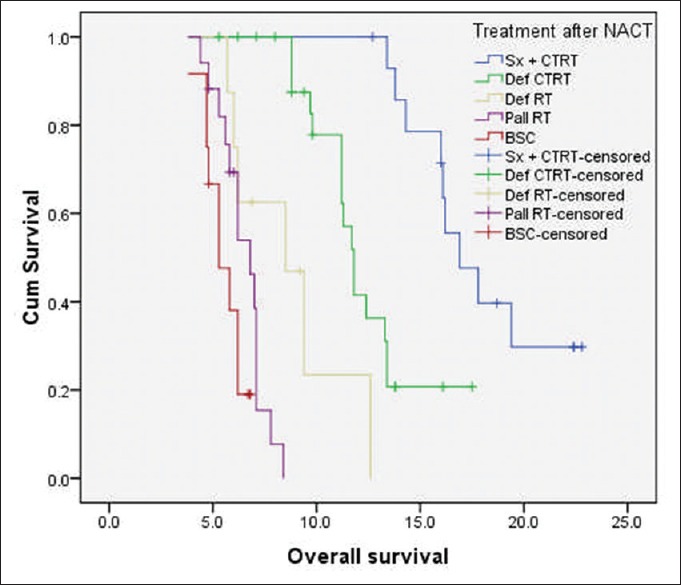
Results: Totally 80 patients received IC, and of them 58 (72.5%) were males. Median age at diagnosis was 44 years (range, 34-62 years). All our patients received IC with doublet regimen. Majority of the patients had buccal mucosa cancers (73.8%), followed by gingivobuccal complex (21.2%) and oral tongue (5%) primaries. After IC, partial response was achieved in 17 (21.3%) patients, stable disease in 49 (61.3%) patients and disease progression was noted in 14 (17.4%) patients. Post-IC, resectability was achieved in 19 (23.8%) of 80 patients, but 4 of them did not undergo surgery due to logistic and personal reasons. The median OS of patients who underwent surgery followed by adjuvant local therapy (n = 15) was 16.9 months (95% CI: 15.2-19.8 months) and for those treated with nonsurgical local therapy (n = 65) was 8.8 months (95% CI: 6.8-10.6 months) (log-rank P = 0.000).
Conclusions: IC had a manageable toxicity profile and achieved resectability in 23.8% of our patients with technically unresectable T4a OSCC. Patients underwent resection had a significantly better median OS than those who received nonsurgical local treatment.
Keywords: Induction chemotherapy; oral cavity squamous cell cancers; technically unresectable.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Induction chemotherapy in locally advanced T4b oral cavity squamous cell cancers: A regional cancer center experience.Indian J Cancer. 2017 Jan-Mar;54(1):35-38. doi: 10.4103/ijc.IJC_131_17. Indian J Cancer. 2017. PMID: 29199659
-
Induction chemotherapy in technically unresectable locally advanced oral cavity cancers: does it make a difference?Indian J Cancer. 2013 Jan-Mar;50(1):1-8. doi: 10.4103/0019-509X.112263. Indian J Cancer. 2013. PMID: 23713035
-
Neoadjuvant chemotherapy followed by surgery in very locally advanced technically unresectable oral cavity cancers.Oral Oncol. 2014 Oct;50(10):1000-4. doi: 10.1016/j.oraloncology.2014.07.015. Epub 2014 Aug 15. Oral Oncol. 2014. PMID: 25130412
-
Management and outcome of locally advanced oral squamous cell carcinoma.Natl J Maxillofac Surg. 2023 May-Aug;14(2):185-189. doi: 10.4103/njms.njms_125_22. Epub 2023 Jul 13. Natl J Maxillofac Surg. 2023. PMID: 37661995 Free PMC article. Review.
-
Neoadjuvant chemotherapy in oral cancers: Selecting the right patients.Indian J Med Paediatr Oncol. 2015 Jul-Sep;36(3):148-53. doi: 10.4103/0971-5851.166716. Indian J Med Paediatr Oncol. 2015. PMID: 26855522 Free PMC article. Review.
Cited by
-
Therapeutic Options in Unresectable Oral Squamous Cell Carcinoma: A Systematic Review.Cancer Manag Res. 2021 Aug 25;13:6705-6719. doi: 10.2147/CMAR.S283204. eCollection 2021. Cancer Manag Res. 2021. PMID: 34471384 Free PMC article. Review.
-
Clinical efficacy of highly agglutinative staphylococcin combined with neoadjuvant chemotherapy on patients with intermediate or advanced oral cancer.Pak J Med Sci. 2022 Sep-Oct;38(7):1973-1979. doi: 10.12669/pjms.38.7.5323. Pak J Med Sci. 2022. PMID: 36246715 Free PMC article.
-
Epidemiology, Diagnostics, and Therapy of Oral Cancer-Update Review.Cancers (Basel). 2024 Sep 14;16(18):3156. doi: 10.3390/cancers16183156. Cancers (Basel). 2024. PMID: 39335128 Free PMC article. Review.
-
Locally Advanced Oral Cavity Cancers: What Is The Optimal Care?Cancer Control. 2020 Jan-Dec;27(1):1073274820920727. doi: 10.1177/1073274820920727. Cancer Control. 2020. PMID: 32339002 Free PMC article. Review.
-
Induction Chemotherapy for Advanced Oral Cavity Cancer.Curr Oncol Rep. 2021 Aug 27;23(11):129. doi: 10.1007/s11912-021-01119-6. Curr Oncol Rep. 2021. PMID: 34453267 Review.
References
-
- Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45:301–8. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin. 2002;52:195–215. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers, Version 2. 2016. [Last accessed on 2016 Nov 17]. Available from: http://www.nccn.org/professionals/physician_gls/pdf/headandneck.pdf .
LinkOut - more resources
Full Text Sources
Other Literature Sources
