

Relationship between growth and illness, enteropathogens and dietary intakes in the first 2 years of life: findings from the MAL-ED birth cohort study
- PMID: 29333282
- PMCID: PMC5759708
- DOI: 10.1136/bmjgh-2017-000370
Relationship between growth and illness, enteropathogens and dietary intakes in the first 2 years of life: findings from the MAL-ED birth cohort study
Abstract
Background: Dietary and illness factors affect risk of growth faltering; the role of enteropathogens is less clear. As part of the Etiology, Risk Factors and Interactions of Enteric Infections and Malnutrition and the Consequences for Child Health and Development (MAL-ED) study, we quantify the effects of enteropathogen infection, diarrhoea and diet on child growth.
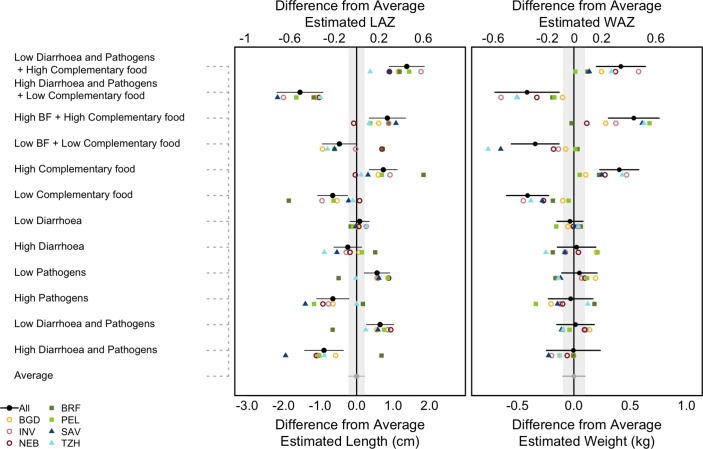
Methods: Newborns were enrolled and followed until 24 months. Length and weight were assessed monthly. Illnesses and breastfeeding practices were documented biweekly; from 9 to 24 months, non-breast milk intakes were quantified monthly. Routinely collected non-diarrhoeal stools were analysed for a broad array of enteropathogens. A linear piecewise spline model was used to quantify associations of each factor with growth velocity in seven of eight MAL-ED sites; cumulative effects on attained size at 24 months were estimated for mean, low (10th percentile) and high (90th percentile) exposure levels. Additionally, the six most prevalent enteropathogens were evaluated for their effects on growth.
Results: Diarrhoea did not have a statistically significant effect on growth. Children with high enteropathogen exposure were estimated to be 1.21±0.33 cm (p<0.001; 0.39 length for age (LAZ)) shorter and 0.08±0.15 kg (p=0.60; 0.08 weight-for-age (WAZ)) lighter at 24 months, on average, than children with low exposure. Campylobacter and enteroaggregativeEscherichia coli detections were associated with deficits of 0.83±0.33 and 0.85±0.31 cm in length (p=0.011 and 0.001) and 0.22±0.15 and 0.09±0.14 kg in weight (p=0.14 and 0.52), respectively. Children with low energy intakes and protein density were estimated to be 1.39±0.33 cm (p<0.001; 0.42 LAZ) shorter and 0.81±0.15 kg (p<0.001; 0.65 WAZ) lighter at 24 months than those with high intakes.
Conclusions: Reducing enteropathogen burden and improving energy and protein density of complementary foods could reduce stunting.
Keywords: child health; cohort study; environmental health; nutritional and metabolic disorders; pneumonia.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- United Nations Children’s Fund. Strategy for improved nutrition of children and women in developing countries. New York, USA: United Nations Children’s Fund, 1990. - PubMed
-
- Scrimshaw NS, Taylor CE, Gordon JE. Interactions of nutrition and infection. Monogr Ser World Health Organ 1968;57:3–329. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials