

Long-term outcomes after Natural Orifice Specimen Extraction versus conventional laparoscopy-assisted surgery for rectal cancer: a matched case-control study
- PMID: 29333423
- PMCID: PMC5765275
- DOI: 10.4174/astr.2018.94.1.26
Long-term outcomes after Natural Orifice Specimen Extraction versus conventional laparoscopy-assisted surgery for rectal cancer: a matched case-control study
Abstract
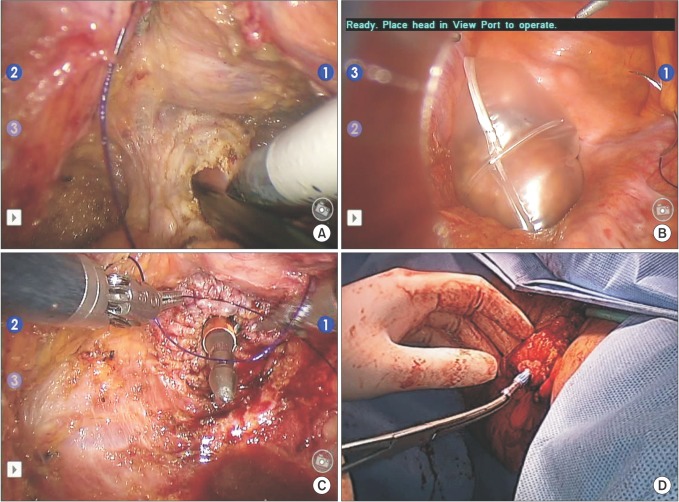
Purpose: The aim of this study was to compare the long-term outcomes of total laparoscopic surgery with Natural Orifice Specimen Extraction (NOSE) with those for conventional laparoscopy (CL)-assisted surgery for treating rectal cancers.
Methods: We reviewed the prospectively collected records of 844 patients (163 NOSE and 681 CL) who underwent curative surgery for mid- or upper rectal cancers from January 2006 to November 2012. We applied propensity score analyses and compared oncological outcomes for the NOSE and CL groups in a 1:1 matched cohort.
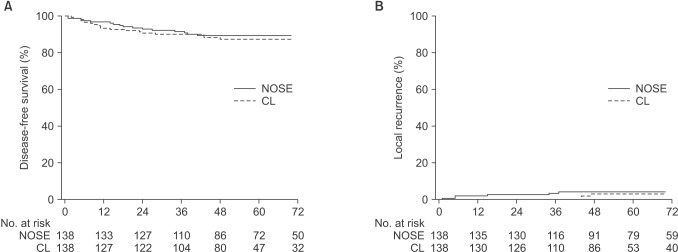
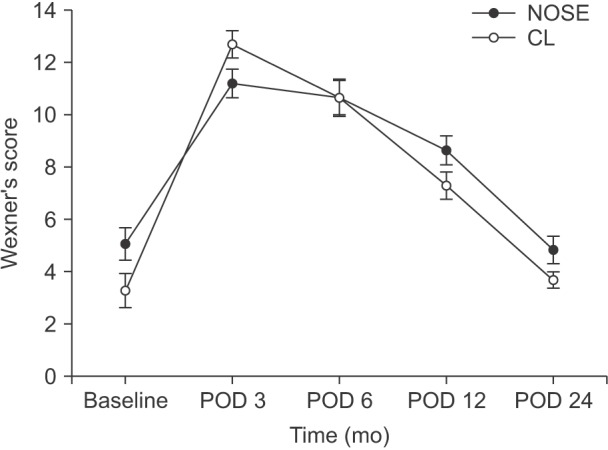
Results: After propensity score matching, each group included 138 patients; the NOSE and CL groups did not differ significantly in terms of baseline clinical characteristics. The median follow-up was 57.7 months (interquartile range, 42.4-82.5 months). The combined 5-year local recurrence rate for all tumor stages was 4.1% (95% confidence interval [CI], 0.9%-7.4%) in the NOSE group and 3.0% (95% CI, 0%-6.3%) in the CL group (P = 0.355). The combined 5-year disease-free survival rates for all stages were 89.3% (95% CI, 84.3%-94.3%) in the NOSE group and 87.3% (95% CI, 81.8%-92.9%) in the CL group (P = 0.639). The postoperative mean fecal incontinence scores at 6, 12, and 24 months were similar between the 2 groups.
Conclusion: In our experience, NOSE for mid- and upper rectal cancer had acceptable long-term oncologic outcomes comparable to those of conventional minimal invasive surgery and seems to be a safe alternative to reduce access trauma.
Keywords: Laparoscopy; Natural Orifice Endoscopic Surgery; Rectal cancer; Survival.
Conflict of interest statement
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Long-term Oncologic Outcomes of Laparoscopic Anterior Resections for Cancer with Natural Orifice Versus Conventional Specimen Extraction: A Case-Control Study.Dis Colon Rectum. 2020 Aug;63(8):1071-1079. doi: 10.1097/DCR.0000000000001622. Dis Colon Rectum. 2020. PMID: 32692072
-
Natural orifice versus conventional mini-laparotomy for specimen extraction after reduced-port laparoscopic surgery for colorectal cancer: propensity score-matched comparative study.Surg Endosc. 2022 Jan;36(1):155-166. doi: 10.1007/s00464-020-08250-8. Epub 2021 Feb 2. Surg Endosc. 2022. PMID: 33532930
-
Outcomes after natural orifice extraction vs conventional specimen extraction surgery for colorectal cancer: A propensity score-matched analysis.World J Clin Oncol. 2022 Oct 24;13(10):789-801. doi: 10.5306/wjco.v13.i10.789. World J Clin Oncol. 2022. PMID: 36337314 Free PMC article.
-
Safety and Oncological Outcomes of Laparoscopic NOSE Surgery Compared With Conventional Laparoscopic Surgery for Colorectal Diseases: A Meta-Analysis.Front Oncol. 2019 Jul 3;9:597. doi: 10.3389/fonc.2019.00597. eCollection 2019. Front Oncol. 2019. PMID: 31334119 Free PMC article.
-
Natural Orifice Specimen Extraction for Right-Sided Colon Cancer: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies.Cureus. 2025 May 15;17(5):e84191. doi: 10.7759/cureus.84191. eCollection 2025 May. Cureus. 2025. PMID: 40376134 Free PMC article. Review.
Cited by
-
The safety and efficacy of laparoscopic surgery versus laparoscopic NOSE for sigmoid and rectal cancer.Surg Endosc. 2022 Jan;36(1):222-235. doi: 10.1007/s00464-020-08260-6. Epub 2021 Jan 21. Surg Endosc. 2022. PMID: 33475847
-
Colorectal resection via natural orifice specimen extraction versus conventional laparoscopic extraction: a meta-analysis with meta-regression.Tech Coloproctol. 2021 Jan;25(1):35-48. doi: 10.1007/s10151-020-02330-6. Epub 2020 Aug 26. Tech Coloproctol. 2021. PMID: 32851500 Review.
-
Development and prospects of natural orifice specimen extraction surgery for colorectal cancer: a review article.Int J Surg. 2025 Apr 1;111(4):2973-2989. doi: 10.1097/JS9.0000000000002285. Int J Surg. 2025. PMID: 39903566 Free PMC article. Review.
-
Carbon nanoparticle-assisted natural orifice specimen extraction surgery with left colic artery preservation: a retrospective study.Wideochir Inne Tech Maloinwazyjne. 2022 Sep;17(3):498-505. doi: 10.5114/wiitm.2022.116284. Epub 2022 May 13. Wideochir Inne Tech Maloinwazyjne. 2022. PMID: 36187060 Free PMC article.
-
Advancing mid-rectal cancer surgery: Unveiling the potential of natural orifice specimen extraction surgery in comparison to conventional laparoscopic-assisted resection.Cancer Rep (Hoboken). 2024 May;7(5):e2003. doi: 10.1002/cnr2.2003. Cancer Rep (Hoboken). 2024. PMID: 38703000 Free PMC article.
References
-
- Bonjer HJ, Deijen CL, Abis GA, Cuesta MA, van der Pas MH, de Lange-de Klerk ES, et al. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;372:1324–1332. - PubMed
-
- Jeong SY, Park JW, Nam BH, Kim S, Kang SB, Lim SB, et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. 2014;15:767–774. - PubMed
-
- Park JS, Choi GS, Jun SH, Park SY, Kim HJ. Long-term outcomes after laparoscopic surgery versus open surgery for rectal cancer: a propensity score analysis. Ann Surg Oncol. 2013;20:2633–2640. - PubMed
-
- Singh R, Omiccioli A, Hegge S, McKinley C. Does the extraction-site location in laparoscopic colorectal surgery have an impact on incisional hernia rates? Surg Endosc. 2008;22:2596–2600. - PubMed
-
- Winslow ER, Fleshman JW, Birnbaum EH, Brunt LM. Wound complications of laparoscopic vs open colectomy. Surg Endosc. 2002;16:1420–1425. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
