

Differential diagnosis and management of placental polyp and uterine arteriovenous malformation: Case reports and review of the literature
- PMID: 29334028
- PMCID: PMC5373263
- DOI: 10.1177/1745505717692590
Differential diagnosis and management of placental polyp and uterine arteriovenous malformation: Case reports and review of the literature
Abstract
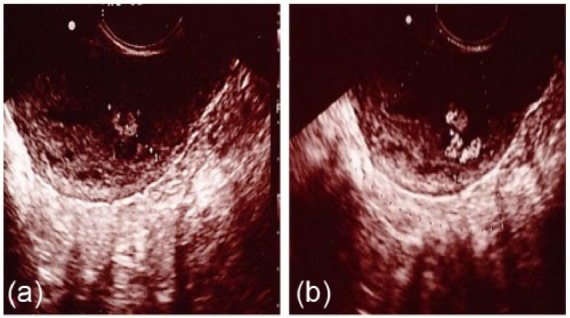
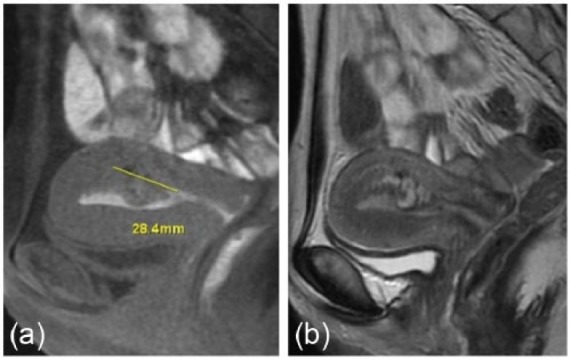
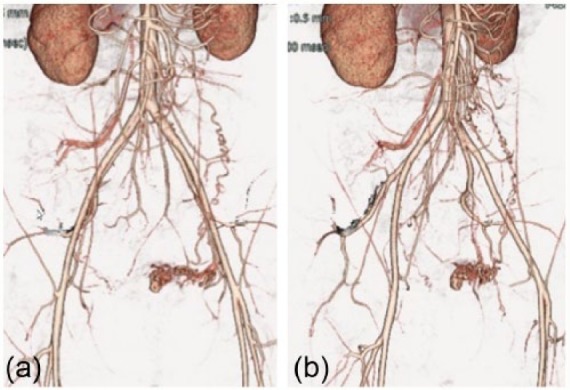
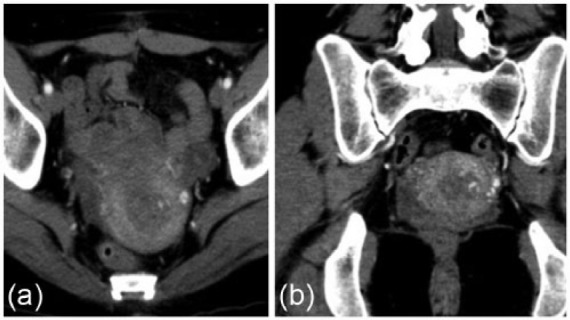
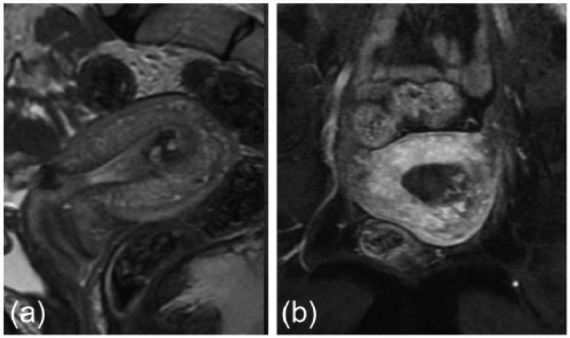
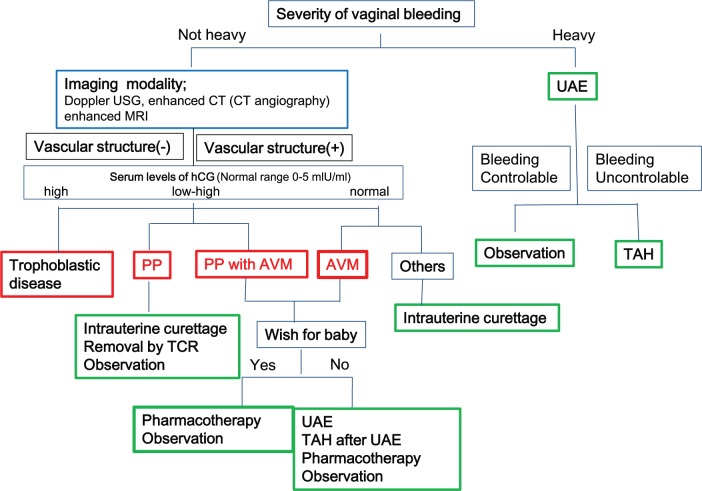
Postpartum uterine bleeding is not uncommon and is caused by a variety of obstetrical and gynecological disorders, such as retained placenta, dysfunctional bleeding, and endometrial polyps. Placental polyps and uterine arteriovenous malformation are disorders often encountered in cases of abnormal uterine bleeding in the late puerperal period. These patients may experience life-threatening bleeding and require prompt intervention based on the correct differential diagnosis. The optimal treatments for both diseases differ as follows: intrauterine curettage or transcervical resection are chosen for placental polyps, while total abdominal hysterectomy or uterine artery embolization is preferred for uterine arteriovenous malformation since intrauterine curettage or transcervical resection has the risk of massive bleeding. However, since placental polyp and uterine arteriovenous malformation have similar clinical characteristics, it is important to accurately identify and differentiate between them to ensure optimal therapy. We report here cases that were suggestive of placental polyp or uterine arteriovenous malformation. We discuss the differential diagnoses and treatments for both diseases based on a literature review and propose a novel algorithm for managing such patients.
Keywords: arteriovenous malformation; diagnosis; placental polyp; transcervical resection; treatment.
Conflict of interest statement
Figures

References
-
- Cunningham FG. Williams obstetrics. 23rd ed. New York: McGraw-Hill, 2010, p. 648.
-
- Swan RW, Woodruff JD. Retained products of conception. Histologic viability of placental polyps. Obstet Gynecol 1969; 34(4): 506–514. - PubMed
-
- Takeda A, Koyama K, Imoto S, et al. Placental polyp with prominent neovascularization. Fertil Steril 2010; 93(4): 1324–1326. - PubMed
-
- Marques K, Looney C, Hayslip C, et al. Modern management of hypervascular placental polypoid mass following spontaneous abortion: a case report and literature review. Am J Obstet Gynecol 2011; 205(2): e9–e11. - PubMed
-
- Fleming H, Ostor AG, Pickel H, et al. Arteriovenous malformations of the uterus. Obstet Gynecol 1989; 73(2): 209–214. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
